Romain L'Huillier, Gilles Poncet, Arnaud Pasquer, Thomas Walter, Catherine Lombard-Bohas, Valérie Hervieu, Bénédicte Cayot, Pierre-Jean Valette, Helen Cheung, Laurent Milot
{"title":"Surgical planning of small intestine neuroendocrine tumors: the concept of mesenteric tumor deposits.","authors":"Romain L'Huillier, Gilles Poncet, Arnaud Pasquer, Thomas Walter, Catherine Lombard-Bohas, Valérie Hervieu, Bénédicte Cayot, Pierre-Jean Valette, Helen Cheung, Laurent Milot","doi":"10.1530/EO-24-0056","DOIUrl":null,"url":null,"abstract":"<p><p>The mesenteric extension of small neuroendocrine tumors is the surgical limiting factor because of the risk of postoperative short bowel syndrome due to superior mesenteric artery involvement. Recent pathological studies have shown that this vascular involvement is due to mesenteric tumor deposits, differentiated from lymph node metastases. The aim of this study was to evaluate the performances of computed tomography (CT) for the surgical planning of small intestine neuroendocrine tumors. This was a retrospective observational study, and all patients undergoing surgery for small intestine neuroendocrine tumor between January 2014 and March 2019 were included. Preoperative CTs were reviewed, blinded from surgical and pathological data, by two radiologists. Diagnostic accuracy and interobserver reliability analysis were performed. We included 45 patients (mean age: 61 years (28-84 years); 23 men). The CT sensitivity to identify the mesenteric mass was 97% (37/38) with a <i>ĸ</i> of 0.73. The positive predictive value of CT to anticipate a right colic resection was 86% (18/21). The negative predictive value of CT was high (97% (34/35) to 100% (35/35)) for duodenal resection (<i>ĸ</i> = 0.78). Regarding retropancreatic lymph node invasion, the CT sensitivity was poor (24%, 4/17), with a high <i>ĸ</i> (0.88). The level of involvement by the mesenteric mass was correlated with the length and the percentage of the remaining small bowel. CT is essential for the surgical planning of small intestine neuroendocrine tumors, being accurate in defining the mesenteric tumor deposits, allowing one to anticipate, with a good reproducibility, the length and percentage of the remaining small bowel and the necessity for a right colectomy.</p>","PeriodicalId":72907,"journal":{"name":"Endocrine oncology (Bristol, England)","volume":"5 1","pages":"e240056"},"PeriodicalIF":0.0000,"publicationDate":"2025-02-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11825162/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrine oncology (Bristol, England)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/EO-24-0056","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
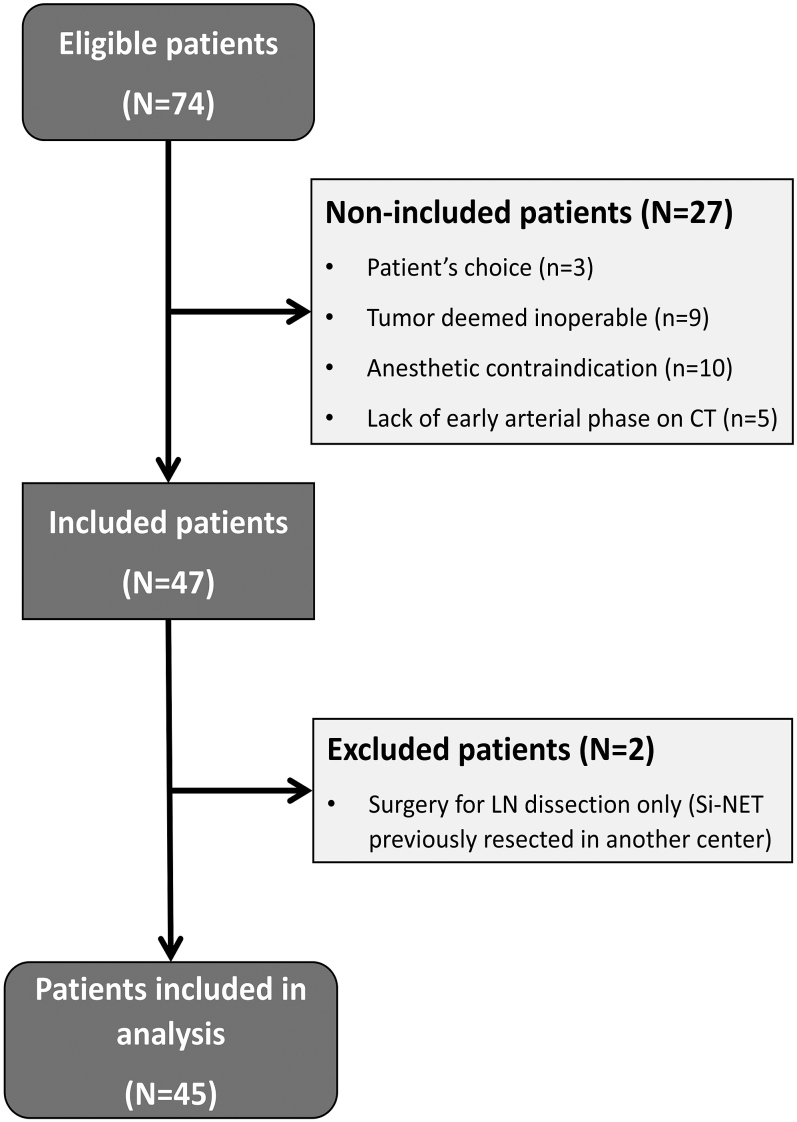
The mesenteric extension of small neuroendocrine tumors is the surgical limiting factor because of the risk of postoperative short bowel syndrome due to superior mesenteric artery involvement. Recent pathological studies have shown that this vascular involvement is due to mesenteric tumor deposits, differentiated from lymph node metastases. The aim of this study was to evaluate the performances of computed tomography (CT) for the surgical planning of small intestine neuroendocrine tumors. This was a retrospective observational study, and all patients undergoing surgery for small intestine neuroendocrine tumor between January 2014 and March 2019 were included. Preoperative CTs were reviewed, blinded from surgical and pathological data, by two radiologists. Diagnostic accuracy and interobserver reliability analysis were performed. We included 45 patients (mean age: 61 years (28-84 years); 23 men). The CT sensitivity to identify the mesenteric mass was 97% (37/38) with a ĸ of 0.73. The positive predictive value of CT to anticipate a right colic resection was 86% (18/21). The negative predictive value of CT was high (97% (34/35) to 100% (35/35)) for duodenal resection (ĸ = 0.78). Regarding retropancreatic lymph node invasion, the CT sensitivity was poor (24%, 4/17), with a high ĸ (0.88). The level of involvement by the mesenteric mass was correlated with the length and the percentage of the remaining small bowel. CT is essential for the surgical planning of small intestine neuroendocrine tumors, being accurate in defining the mesenteric tumor deposits, allowing one to anticipate, with a good reproducibility, the length and percentage of the remaining small bowel and the necessity for a right colectomy.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


