Mahesh Nagappa, Yamini Subramani, Homer Yang, Natasha Wood, Jill Querney, Lee-Anne Fochesato, Derek Nguyen, Nida Fatima, Janet Martin, Ava John-Baptiste, Rahul Nayak, Mehdi Qiabi, Richard Inculet, Dalilah Fortin, Richard Malthaner
{"title":"Enhancing Quadruple Health Outcomes After Thoracic Surgery: Feasibility Pilot Randomized Controlled Trial Using Digital Home Monitoring.","authors":"Mahesh Nagappa, Yamini Subramani, Homer Yang, Natasha Wood, Jill Querney, Lee-Anne Fochesato, Derek Nguyen, Nida Fatima, Janet Martin, Ava John-Baptiste, Rahul Nayak, Mehdi Qiabi, Richard Inculet, Dalilah Fortin, Richard Malthaner","doi":"10.2196/58998","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Surgical recovery after hospital discharge often presents challenges for patients and caregivers. Postoperative complications and poorly managed pain at home can lead to unexpected visits to the emergency department (ED) and readmission to the hospital. Digital home monitoring (DHM) may improve postoperative care compared to standard methods.</p><p><strong>Objective: </strong>We conducted a feasibility study for a randomized controlled trial (RCT) to assess DHM's effectiveness following thoracic surgical procedures compared to standard care.</p><p><strong>Methods: </strong>We conducted a 2-arm parallel-group pilot RCT at a single tertiary care center. Adult patients undergoing thoracic surgical procedures were randomized 1:1 into 2 groups: the DHM group and the standard of care (control group). We adhered to the intention-to-treat analysis principle. The primary outcome was predetermined RCT feasibility criteria. The trial would be feasible if more than 75% of trial recruitment, protocol adherence, and data collection were achieved. Secondary outcomes included 30-day ED visit rates, 30-day readmission rates, postoperative complications, length of stay, postdischarge 30-day opioid consumption, 30-day quality of recovery, patient-program satisfaction, caregiver satisfaction, health care provider satisfaction, and cost per case.</p><p><strong>Results: </strong>All RCT feasibility criteria were met. The trial recruitment rate was 87.9% (95% CI 79.4%-93.8%). Protocol adherence and outcome data collection rates were 96.3% (95% CI 89.4%-99.2%) and 98.7% (95% CI 92.9%-99.9%), respectively. In total, 80 patients were randomized, with 40 (50%) in the DHM group and 40 (50%) in the control group. Baseline patient and clinical characteristics were comparable between the 2 groups. The DHM group had fewer unplanned ED visits (2.7% vs 20.5%; P=.02), fewer unplanned admission rates (0% vs 7.6%; P=.24), lower rates of postoperative complications (20% vs 47.5%, P=.01) shorter hospital stays (4.0 vs 6.9 days; P=.05), but more opioid consumption (111.6, SD 110.9) vs 74.3, SD 71.9 mg morphine equivalents; P=.08) compared to the control group. DHM also resulted in shorter ED visit times (130, SD 0 vs 1048, SD 1093 minutes; P=.48) and lower cost per case (CAD $12,145 [US $ 8436.34], SD CAD $8779 [US $ 6098.20] vs CAD $17,247 [US $11,980.37], SD CAD $15,313 [US $10,636.95]; P=.07). The quality of recovery scores was clinically significantly better than the controls (185.4, SD 2.6 vs 178.3, SD 3.3; P<.001). All 37 patients who completed the intervention answered the program satisfaction survey questionnaires (100%; 95% CI 90.5%-100%). Only 36 out of 80 caregivers responded to the caregiver satisfaction questionnaires at the end of the fourth week post hospital discharge (47.7%; 95% CI 35.7%-59.1%). Health care providers reported a 100% satisfaction rate.</p><p><strong>Conclusions: </strong>This pilot RCT demonstrates the feasibility of conducting a full-scale trial to assess DHM's efficacy in improving postoperative care following thoracic surgery. DHM shows promise for enhancing continuity of care and warrants further investigation.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov NCT04340960; https://clinicaltrials.gov/study/NCT04340960.</p>","PeriodicalId":73557,"journal":{"name":"JMIR perioperative medicine","volume":"8 ","pages":"e58998"},"PeriodicalIF":0.0000,"publicationDate":"2025-02-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11888079/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR perioperative medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/58998","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Surgical recovery after hospital discharge often presents challenges for patients and caregivers. Postoperative complications and poorly managed pain at home can lead to unexpected visits to the emergency department (ED) and readmission to the hospital. Digital home monitoring (DHM) may improve postoperative care compared to standard methods.
Objective: We conducted a feasibility study for a randomized controlled trial (RCT) to assess DHM's effectiveness following thoracic surgical procedures compared to standard care.
Methods: We conducted a 2-arm parallel-group pilot RCT at a single tertiary care center. Adult patients undergoing thoracic surgical procedures were randomized 1:1 into 2 groups: the DHM group and the standard of care (control group). We adhered to the intention-to-treat analysis principle. The primary outcome was predetermined RCT feasibility criteria. The trial would be feasible if more than 75% of trial recruitment, protocol adherence, and data collection were achieved. Secondary outcomes included 30-day ED visit rates, 30-day readmission rates, postoperative complications, length of stay, postdischarge 30-day opioid consumption, 30-day quality of recovery, patient-program satisfaction, caregiver satisfaction, health care provider satisfaction, and cost per case.
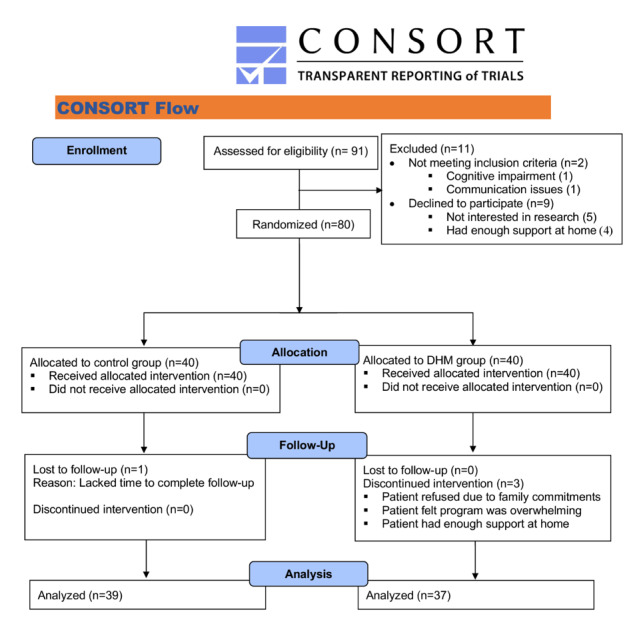
Results: All RCT feasibility criteria were met. The trial recruitment rate was 87.9% (95% CI 79.4%-93.8%). Protocol adherence and outcome data collection rates were 96.3% (95% CI 89.4%-99.2%) and 98.7% (95% CI 92.9%-99.9%), respectively. In total, 80 patients were randomized, with 40 (50%) in the DHM group and 40 (50%) in the control group. Baseline patient and clinical characteristics were comparable between the 2 groups. The DHM group had fewer unplanned ED visits (2.7% vs 20.5%; P=.02), fewer unplanned admission rates (0% vs 7.6%; P=.24), lower rates of postoperative complications (20% vs 47.5%, P=.01) shorter hospital stays (4.0 vs 6.9 days; P=.05), but more opioid consumption (111.6, SD 110.9) vs 74.3, SD 71.9 mg morphine equivalents; P=.08) compared to the control group. DHM also resulted in shorter ED visit times (130, SD 0 vs 1048, SD 1093 minutes; P=.48) and lower cost per case (CAD $12,145 [US $ 8436.34], SD CAD $8779 [US $ 6098.20] vs CAD $17,247 [US $11,980.37], SD CAD $15,313 [US $10,636.95]; P=.07). The quality of recovery scores was clinically significantly better than the controls (185.4, SD 2.6 vs 178.3, SD 3.3; P<.001). All 37 patients who completed the intervention answered the program satisfaction survey questionnaires (100%; 95% CI 90.5%-100%). Only 36 out of 80 caregivers responded to the caregiver satisfaction questionnaires at the end of the fourth week post hospital discharge (47.7%; 95% CI 35.7%-59.1%). Health care providers reported a 100% satisfaction rate.
Conclusions: This pilot RCT demonstrates the feasibility of conducting a full-scale trial to assess DHM's efficacy in improving postoperative care following thoracic surgery. DHM shows promise for enhancing continuity of care and warrants further investigation.
背景:出院后的手术康复对患者和护理人员来说都是一个挑战。术后并发症和家庭疼痛管理不善可能导致意外访问急诊室(ED)和再次入院。与标准方法相比,数字家庭监测(DHM)可以改善术后护理。目的:我们进行了一项随机对照试验(RCT)的可行性研究,以评估与标准治疗相比,胸外科手术后DHM的有效性。方法:我们在一个三级保健中心进行了一项两臂平行组先导随机对照试验。接受胸外科手术的成年患者按1:1随机分为两组:DHM组和标准护理组(对照组)。我们坚持意向治疗分析原则。主要结局是预先确定的RCT可行性标准。如果试验招募率、方案依从性和数据收集达到75%以上,则该试验是可行的。次要结局包括30天急诊科就诊率、30天再入院率、术后并发症、住院时间、出院后30天阿片类药物消耗量、30天康复质量、患者-项目满意度、护理人员满意度、卫生保健提供者满意度和每例费用。结果:符合所有RCT可行性标准。试验招募率为87.9% (95% CI 79.4%-93.8%)。方案依从性和结局数据收集率分别为96.3% (95% CI 89.4%-99.2%)和98.7% (95% CI 92.9%-99.9%)。共随机选取80例患者,DHM组40例(50%),对照组40例(50%)。两组患者的基线和临床特征具有可比性。DHM组计划外急诊科就诊较少(2.7% vs 20.5%;P=.02),非计划入院率较少(0% vs 7.6%;P= 0.24),术后并发症发生率较低(20% vs 47.5%, P= 0.01),住院时间较短(4.0 vs 6.9天;P= 0.05),但更多的阿片类药物消耗(111.6,SD 110.9) vs 74.3, SD 71.9 mg吗啡当量;P=.08)。DHM还缩短了ED就诊时间(130,SD 0 vs 1048, SD 1093分钟);P=.48)和更低的每例成本(12,145加元[8436.34美元],SD $8779加元[6098.20美元]vs 17,247加元[11,980.37美元],SD $15,313加元[10,636.95美元];P = . 07)。恢复评分质量显著优于对照组(185.4,SD 2.6 vs 178.3, SD 3.3;结论:该试点RCT证明了开展全面试验以评估DHM改善胸外科术后护理的有效性的可行性。DHM有望加强护理的连续性,值得进一步调查。试验注册:ClinicalTrials.gov NCT04340960;https://clinicaltrials.gov/study/NCT04340960。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


