Sofia Shoaib, Joseph Feliciano, Elliott C Dasenbrook, Jason Maynard, Lakshmi Batchu, Maitreyee Mohanty, Melanie Lauterio, Alexandra J Feld
{"title":"Real-world disease burden, mortality, and healthcare resource utilization associated with bronchiectasis.","authors":"Sofia Shoaib, Joseph Feliciano, Elliott C Dasenbrook, Jason Maynard, Lakshmi Batchu, Maitreyee Mohanty, Melanie Lauterio, Alexandra J Feld","doi":"10.1177/14799731241310897","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To assess real-world survival and healthcare resource utilization (HCRU) in US patients with non-cystic fibrosis bronchiectasis (NCFBE).</p><p><strong>Methods: </strong>This retrospective analysis, using data from the STATinMED RWD Insights database from Jan 2015-Oct 2022, included adults with NCFBE (from Jan 2015-Oct 2021) and non-NCFBE comparators (from Jan 2015-Aug 2020); baseline characteristics were balanced by inverse probability treatment weighting. Outcomes included survival through end of study. HCRU was assessed over 12 months.</p><p><strong>Results: </strong>117,718 patients with NCFBE and 306,678 comparators were included. Patients with NCFBE had a 77% higher risk of death than comparators (hazard ratio [HR] 1.77 [95% CI 1.74-1.80]). Risk of death was higher among patients aged ≥65 years (vs 18-34 years; HR 11.03 [95% CI 10.36-11.74]), among Black patients (vs White; HR 1.53 [95% CI 1.50-1.55]), and among patients with comorbid COPD (HR 1.42 [95% CI 1.40-1.44]). Patients with NCFBE incurred higher all-cause and respiratory-related HCRU than comparators for outpatient office, outpatient hospital, emergency department (ED), inpatient and respiratory-related pulmonologist visits (all <i>p</i> < .0001); HCRU increased with exacerbations.</p><p><strong>Conclusions: </strong>Patients with NCFBE have high mortality burden and incur high HCRU, both of which are further increased with exacerbations. Prevention and delay of exacerbations are key areas for improvement of disease management.</p>","PeriodicalId":10217,"journal":{"name":"Chronic Respiratory Disease","volume":"22 ","pages":"14799731241310897"},"PeriodicalIF":2.3000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11808752/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chronic Respiratory Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/14799731241310897","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To assess real-world survival and healthcare resource utilization (HCRU) in US patients with non-cystic fibrosis bronchiectasis (NCFBE).
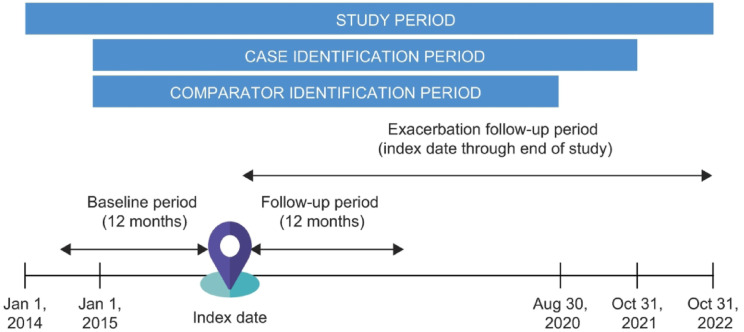
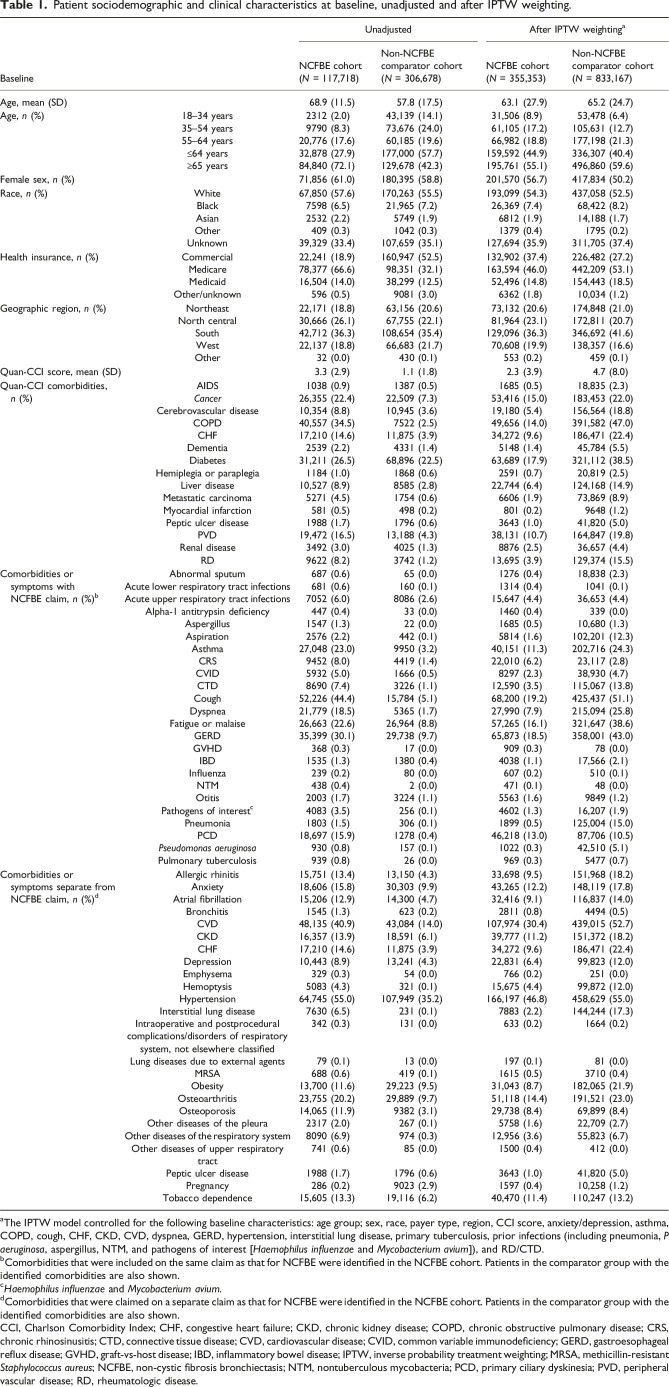
Methods: This retrospective analysis, using data from the STATinMED RWD Insights database from Jan 2015-Oct 2022, included adults with NCFBE (from Jan 2015-Oct 2021) and non-NCFBE comparators (from Jan 2015-Aug 2020); baseline characteristics were balanced by inverse probability treatment weighting. Outcomes included survival through end of study. HCRU was assessed over 12 months.
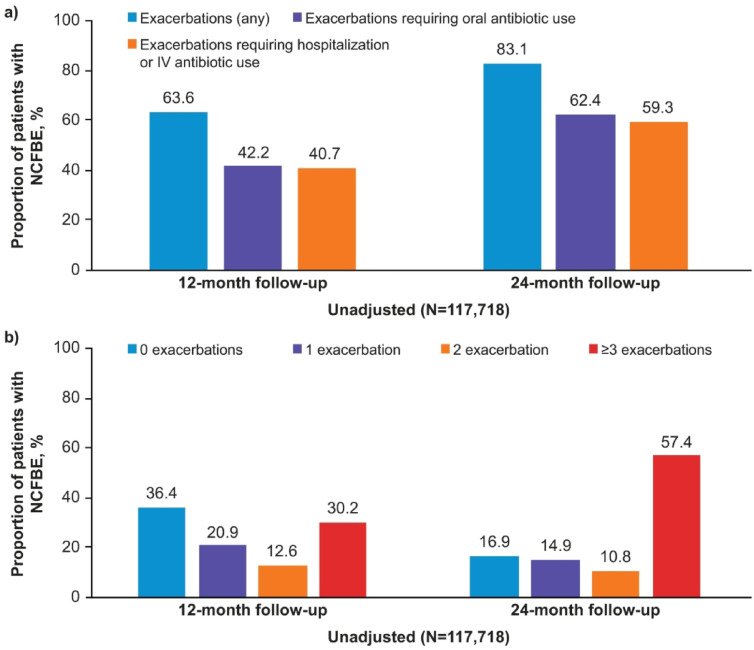
Results: 117,718 patients with NCFBE and 306,678 comparators were included. Patients with NCFBE had a 77% higher risk of death than comparators (hazard ratio [HR] 1.77 [95% CI 1.74-1.80]). Risk of death was higher among patients aged ≥65 years (vs 18-34 years; HR 11.03 [95% CI 10.36-11.74]), among Black patients (vs White; HR 1.53 [95% CI 1.50-1.55]), and among patients with comorbid COPD (HR 1.42 [95% CI 1.40-1.44]). Patients with NCFBE incurred higher all-cause and respiratory-related HCRU than comparators for outpatient office, outpatient hospital, emergency department (ED), inpatient and respiratory-related pulmonologist visits (all p < .0001); HCRU increased with exacerbations.
Conclusions: Patients with NCFBE have high mortality burden and incur high HCRU, both of which are further increased with exacerbations. Prevention and delay of exacerbations are key areas for improvement of disease management.
目的:评估美国非囊性纤维化支气管扩张症(NCFBE)患者的真实生存和医疗资源利用(HCRU)。方法:回顾性分析使用STATinMED RWD Insights数据库2015年1月至2022年10月的数据,包括患有NCFBE的成年人(2015年1月至2021年10月)和非NCFBE比较者(2015年1月至2020年8月);基线特征通过逆概率处理加权来平衡。结果包括研究结束时的生存。HCRU在12个月内进行评估。结果:纳入117,718例NCFBE患者和306,678例比较者。NCFBE患者的死亡风险比对照组高77%(风险比[HR] 1.77 [95% CI 1.74-1.80])。年龄≥65岁的患者死亡风险较高(18-34岁;HR 11.03 [95% CI 10.36-11.74]),黑人患者(vs白人;HR为1.53 [95% CI 1.50-1.55]),合并COPD患者的HR为1.42 [95% CI 1.40-1.44])。非cfbe患者在门诊、医院门诊、急诊科(ED)、住院和呼吸相关肺科就诊的全因和呼吸相关HCRU均高于对照患者(p < 0.0001);HCRU随病情加重而升高。结论:NCFBE患者具有高死亡率负担和高HCRU,且随病情加重而进一步增加。预防和延缓恶化是改善疾病管理的关键领域。
期刊介绍:
Chronic Respiratory Disease is a peer-reviewed, open access, scholarly journal, created in response to the rising incidence of chronic respiratory diseases worldwide. It publishes high quality research papers and original articles that have immediate relevance to clinical practice and its multi-disciplinary perspective reflects the nature of modern treatment. The journal provides a high quality, multi-disciplinary focus for the publication of original papers, reviews and commentary in the broad area of chronic respiratory disease, particularly its treatment and management.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


