{"title":"Predictive Modeling of Symptomatic Intracranial Hemorrhage Following Endovascular Thrombectomy: Insights From the Nationwide TREAT-AIS Registry.","authors":"Jia-Hung Chen, I-Chang Su, Yueh-Hsun Lu, Yi-Chen Hsieh, Chih-Hao Chen, Chun-Jen Lin, Yu-Wei Chen, Kuan-Hung Lin, Pi-Shan Sung, Chih-Wei Tang, Hai-Jui Chu, Chuan-Hsiu Fu, Chao-Liang Chou, Cheng-Yu Wei, Shang-Yih Yan, Po-Lin Chen, Hsu-Ling Yeh, Sheng-Feng Sung, Hon-Man Liu, Ching-Huang Lin, Meng Lee, Sung-Chun Tang, I-Hui Lee, Lung Chan, Li-Ming Lien, Hung-Yi Chiou, Jiunn-Tay Lee, Jiann-Shing Jeng","doi":"10.5853/jos.2024.04119","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>Symptomatic intracranial hemorrhage (sICH) following endovascular thrombectomy (EVT) is a severe complication associated with adverse functional outcomes and increased mortality rates. Currently, a reliable predictive model for sICH risk after EVT is lacking.</p><p><strong>Methods: </strong>This study used data from patients aged ≥20 years who underwent EVT for anterior circulation stroke from the nationwide Taiwan Registry of Endovascular Thrombectomy for Acute Ischemic Stroke (TREAT-AIS). A predictive model including factors associated with an increased risk of sICH after EVT was developed to differentiate between patients with and without sICH. This model was compared existing predictive models using nationwide registry data to evaluate its relative performance.</p><p><strong>Results: </strong>Of the 2,507 identified patients, 158 developed sICH after EVT. Factors such as diastolic blood pressure, Alberta Stroke Program Early CT Score, platelet count, glucose level, collateral score, and successful reperfusion were associated with the risk of sICH after EVT. The TREAT-AIS score demonstrated acceptable predictive accuracy (area under the curve [AUC]=0.694), with higher scores being associated with an increased risk of sICH (odds ratio=2.01 per score increase, 95% confidence interval=1.64-2.45, P<0.001). The discriminatory capacity of the score was similar in patients with symptom onset beyond 6 hours (AUC=0.705). Compared to existing models, the TREAT-AIS score consistently exhibited superior predictive accuracy, although this difference was marginal.</p><p><strong>Conclusion: </strong>s The TREAT-AIS score outperformed existing models, and demonstrated an acceptable discriminatory capacity for distinguishing patients according to sICH risk levels. However, the differences between models were only marginal. Further research incorporating periprocedural and postprocedural factors is required to improve the predictive accuracy.</p>","PeriodicalId":17135,"journal":{"name":"Journal of Stroke","volume":"27 1","pages":"85-94"},"PeriodicalIF":8.6000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11834349/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Stroke","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5853/jos.2024.04119","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/31 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and purpose: Symptomatic intracranial hemorrhage (sICH) following endovascular thrombectomy (EVT) is a severe complication associated with adverse functional outcomes and increased mortality rates. Currently, a reliable predictive model for sICH risk after EVT is lacking.
Methods: This study used data from patients aged ≥20 years who underwent EVT for anterior circulation stroke from the nationwide Taiwan Registry of Endovascular Thrombectomy for Acute Ischemic Stroke (TREAT-AIS). A predictive model including factors associated with an increased risk of sICH after EVT was developed to differentiate between patients with and without sICH. This model was compared existing predictive models using nationwide registry data to evaluate its relative performance.
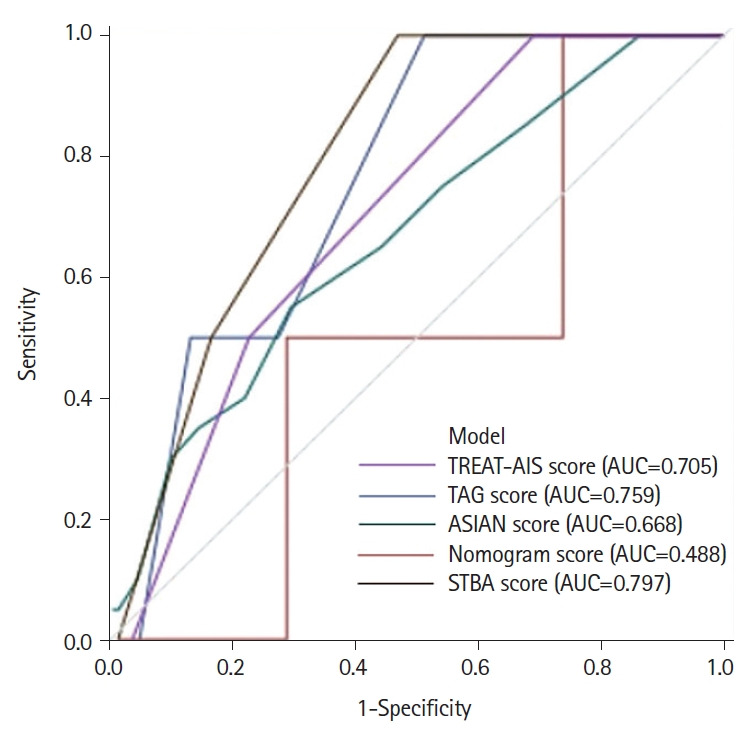
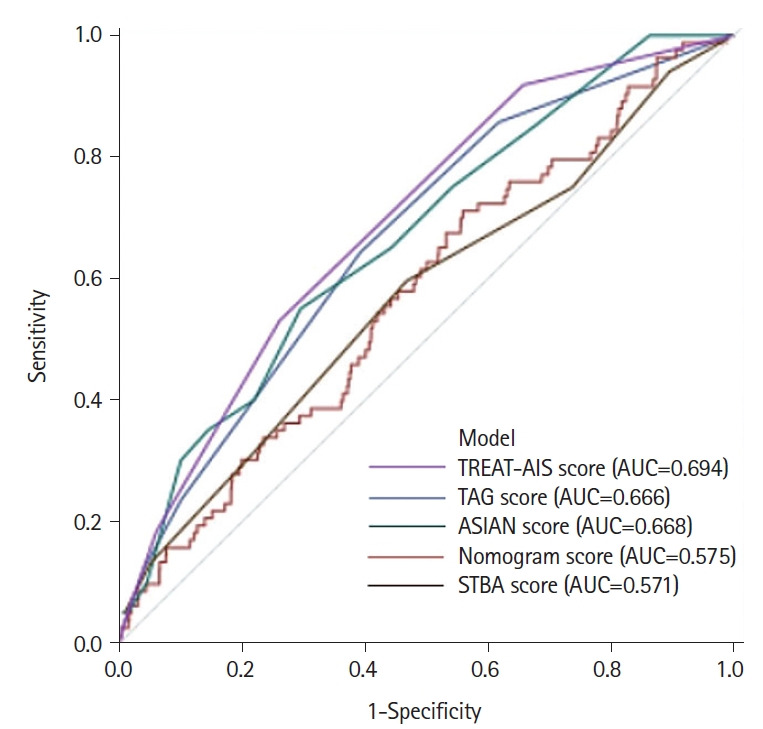
Results: Of the 2,507 identified patients, 158 developed sICH after EVT. Factors such as diastolic blood pressure, Alberta Stroke Program Early CT Score, platelet count, glucose level, collateral score, and successful reperfusion were associated with the risk of sICH after EVT. The TREAT-AIS score demonstrated acceptable predictive accuracy (area under the curve [AUC]=0.694), with higher scores being associated with an increased risk of sICH (odds ratio=2.01 per score increase, 95% confidence interval=1.64-2.45, P<0.001). The discriminatory capacity of the score was similar in patients with symptom onset beyond 6 hours (AUC=0.705). Compared to existing models, the TREAT-AIS score consistently exhibited superior predictive accuracy, although this difference was marginal.
Conclusion: s The TREAT-AIS score outperformed existing models, and demonstrated an acceptable discriminatory capacity for distinguishing patients according to sICH risk levels. However, the differences between models were only marginal. Further research incorporating periprocedural and postprocedural factors is required to improve the predictive accuracy.
Journal of StrokeCLINICAL NEUROLOGYPERIPHERAL VASCULAR DISE-PERIPHERAL VASCULAR DISEASE
CiteScore
11.00
自引率
3.70%
发文量
52
审稿时长
12 weeks
期刊介绍:
The Journal of Stroke (JoS) is a peer-reviewed publication that focuses on clinical and basic investigation of cerebral circulation and associated diseases in stroke-related fields. Its aim is to enhance patient management, education, clinical or experimental research, and professionalism. The journal covers various areas of stroke research, including pathophysiology, risk factors, symptomatology, imaging, treatment, and rehabilitation. Basic science research is included when it provides clinically relevant information. The JoS is particularly interested in studies that highlight characteristics of stroke in the Asian population, as they are underrepresented in the literature.
The JoS had an impact factor of 8.2 in 2022 and aims to provide high-quality research papers to readers while maintaining a strong reputation. It is published three times a year, on the last day of January, May, and September. The online version of the journal is considered the main version as it includes all available content. Supplementary issues are occasionally published.
The journal is indexed in various databases, including SCI(E), Pubmed, PubMed Central, Scopus, KoreaMed, Komci, Synapse, Science Central, Google Scholar, and DOI/Crossref. It is also the official journal of the Korean Stroke Society since 1999, with the abbreviated title J Stroke.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


