Tahazid Tamannur, Sadhan Kumar Das, Arifatun Nesa, Foijun Nahar, Nadia Nowshin, Tasnim Haque Binty, Shafiul Azam Shakil, Shuvojit Kumar Kundu, Md Abu Bakkar Siddik, Shafkat Mahmud Rafsun, Umme Habiba, Zaki Farhana, Hafiza Sultana, Anton Abdulbasah Kamil, Mohammad Meshbahur Rahman
{"title":"Mothers' Knowledge of and Practices Toward Oral Hygiene of Children Aged 5-9 Years in Bangladesh: Cross-Sectional Study.","authors":"Tahazid Tamannur, Sadhan Kumar Das, Arifatun Nesa, Foijun Nahar, Nadia Nowshin, Tasnim Haque Binty, Shafiul Azam Shakil, Shuvojit Kumar Kundu, Md Abu Bakkar Siddik, Shafkat Mahmud Rafsun, Umme Habiba, Zaki Farhana, Hafiza Sultana, Anton Abdulbasah Kamil, Mohammad Meshbahur Rahman","doi":"10.2196/59379","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Healthy oral hygiene is crucial for overall health and well-being. Parents' dental care knowledge and practices affect their children's oral health.</p><p><strong>Objective: </strong>This study examined mothers' knowledge and practices regarding their children's oral hygiene through a cross-sectional survey.</p><p><strong>Methods: </strong>This cross-sectional survey was conducted from January 1 to December 31, 2022, in Dhaka, Bangladesh. Mothers' knowledge and practices regarding their children's oral hygiene were assessed through a semistructured questionnaire. Statistical analyses, including the χ2 test and Pearson correlation test, were performed. The Mann-Whitney U and Kruskal-Wallis 1-way ANOVA tests were also used to show the average variations in knowledge and practices among different sociodemographic groups.</p><p><strong>Results: </strong>Of 400 participants, the mean age of mothers was 30.94 (SD 5.15) years, and 388 (97%) were of the Muslim faith, 347 (86.8%) were housewives, and 272 (68%) came from nuclear families. A total of 165 (41.3%) participants showed good knowledge of their children's oral hygiene, followed by 86 (21.5%) showing moderately average knowledge, 75 (18.8%) showing average knowledge, and 74 (18.5%) showing poor knowledge. A total of 182 (45.5%) mothers had children with good oral hygiene practices, followed by mothers with children who had average (n=78, 19.5%), moderately average (n=75, 18.8%), and poor (n=65, 16.3%) oral hygiene practices. The mother's knowledge level was significantly associated with age (P=.01), education (P<.001), family size (P=.03), and monthly income (P<.001). On the other hand, educational status (P=.002) and income (P=.04) were significantly associated with the mother's practices regarding their children's oral hygiene. Nonparametric analysis revealed that mothers who were older (mean knowledge score: 12.13, 95% CI 10.73-13.54 vs 11.21, 95% CI 10.85-11.58; P=.01), with a bachelor's degree or higher (mean knowledge score: 12.93, 95% CI 12.55-13.31 vs 9.66, 95% CI 8.95-10.37; P<.001), who were working mothers (mean knowledge score: 12.30, 95% CI 11.72-12.89 vs 11.45, 95% CI 11.17-11.73; P=.03), and who had a higher family income (mean knowledge score: 12.49, 95% CI 12.0-12.98 vs 10.92, 95% CI 10.48-11.36; P<.001) demonstrated significantly higher levels of oral health knowledge. Conversely, good oral hygiene practices were significantly associated with higher maternal education (mean practice score: 6.88, 95% CI 6.54-7.22 vs 6.01, 95% CI 5.63-6.40; P<.001) and family income (mean practice score: 6.77, 95% CI 6.40-7.14 vs 5.96, 95% CI 5.68-6.24; P=.002). The mother's knowledge was also significantly and positively correlated (Pearson correlation coefficient r=0.301; P<.001) with their children's oral hygiene practices, shown by both the Pearson chi-square (χ2=25.2; P<.001) test and correlation coefficient.</p><p><strong>Conclusions: </strong>The mothers' knowledge and their children's oral hygiene practices were inadequate. The mother's age, education level, family size, and monthly income significantly influenced their knowledge level. Children's oral hygiene habits were significantly associated with family income and the mother's educational status. This underscores the need for educational programs, accessible dental care services, oral health education in the curriculum, media and technology involvement in oral health educational campaigns, and proper research and monitoring.</p>","PeriodicalId":73558,"journal":{"name":"JMIRx med","volume":"6 ","pages":"e59379"},"PeriodicalIF":0.0000,"publicationDate":"2025-02-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11809941/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIRx med","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/59379","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Healthy oral hygiene is crucial for overall health and well-being. Parents' dental care knowledge and practices affect their children's oral health.
Objective: This study examined mothers' knowledge and practices regarding their children's oral hygiene through a cross-sectional survey.
Methods: This cross-sectional survey was conducted from January 1 to December 31, 2022, in Dhaka, Bangladesh. Mothers' knowledge and practices regarding their children's oral hygiene were assessed through a semistructured questionnaire. Statistical analyses, including the χ2 test and Pearson correlation test, were performed. The Mann-Whitney U and Kruskal-Wallis 1-way ANOVA tests were also used to show the average variations in knowledge and practices among different sociodemographic groups.
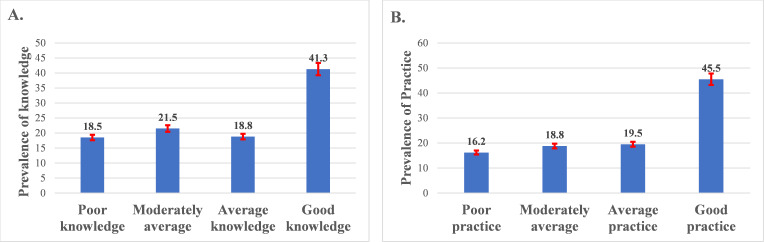
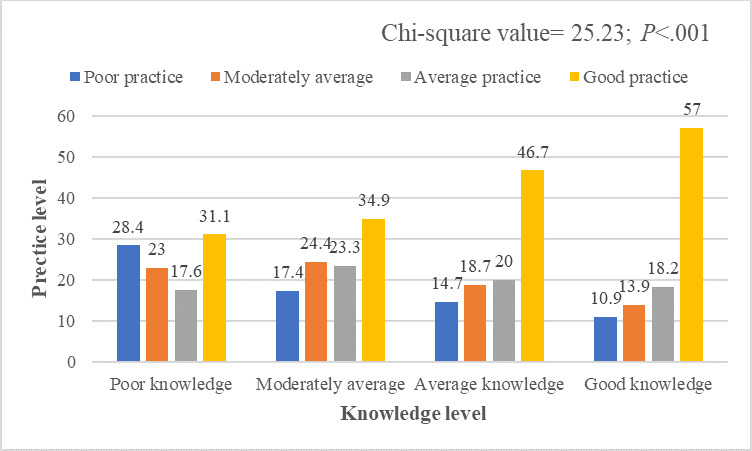
Results: Of 400 participants, the mean age of mothers was 30.94 (SD 5.15) years, and 388 (97%) were of the Muslim faith, 347 (86.8%) were housewives, and 272 (68%) came from nuclear families. A total of 165 (41.3%) participants showed good knowledge of their children's oral hygiene, followed by 86 (21.5%) showing moderately average knowledge, 75 (18.8%) showing average knowledge, and 74 (18.5%) showing poor knowledge. A total of 182 (45.5%) mothers had children with good oral hygiene practices, followed by mothers with children who had average (n=78, 19.5%), moderately average (n=75, 18.8%), and poor (n=65, 16.3%) oral hygiene practices. The mother's knowledge level was significantly associated with age (P=.01), education (P<.001), family size (P=.03), and monthly income (P<.001). On the other hand, educational status (P=.002) and income (P=.04) were significantly associated with the mother's practices regarding their children's oral hygiene. Nonparametric analysis revealed that mothers who were older (mean knowledge score: 12.13, 95% CI 10.73-13.54 vs 11.21, 95% CI 10.85-11.58; P=.01), with a bachelor's degree or higher (mean knowledge score: 12.93, 95% CI 12.55-13.31 vs 9.66, 95% CI 8.95-10.37; P<.001), who were working mothers (mean knowledge score: 12.30, 95% CI 11.72-12.89 vs 11.45, 95% CI 11.17-11.73; P=.03), and who had a higher family income (mean knowledge score: 12.49, 95% CI 12.0-12.98 vs 10.92, 95% CI 10.48-11.36; P<.001) demonstrated significantly higher levels of oral health knowledge. Conversely, good oral hygiene practices were significantly associated with higher maternal education (mean practice score: 6.88, 95% CI 6.54-7.22 vs 6.01, 95% CI 5.63-6.40; P<.001) and family income (mean practice score: 6.77, 95% CI 6.40-7.14 vs 5.96, 95% CI 5.68-6.24; P=.002). The mother's knowledge was also significantly and positively correlated (Pearson correlation coefficient r=0.301; P<.001) with their children's oral hygiene practices, shown by both the Pearson chi-square (χ2=25.2; P<.001) test and correlation coefficient.
Conclusions: The mothers' knowledge and their children's oral hygiene practices were inadequate. The mother's age, education level, family size, and monthly income significantly influenced their knowledge level. Children's oral hygiene habits were significantly associated with family income and the mother's educational status. This underscores the need for educational programs, accessible dental care services, oral health education in the curriculum, media and technology involvement in oral health educational campaigns, and proper research and monitoring.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


