{"title":"CHA<sub>2</sub>DS<sub>2</sub>-VASc Score Is Associated With Prognosis in Patients With Acute Ischemic Stroke Without Atrial Fibrillation.","authors":"Mingjuan Song, Xu Chen","doi":"10.14503/THIJ-24-8450","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Although the prognostic value of the CHA<sub>2</sub>DS<sub>2</sub>-VASc (congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, prior stroke or transient ischemic attack, vascular disease, age 65-74 years, and female sex) scoring system in patients with stroke has been explored in several studies, a research gap exists in its application, especially in patients without atrial fibrillation (AF).</p><p><strong>Methods: </strong>This study investigated the association between CHA<sub>2</sub>DS<sub>2</sub>-VASc score and prognosis at 1 year in patients with acute ischemic stroke (AIS) who do not have AF. A total of 993 patients with AIS but without AF were recruited between January 2019 and December 2022. Patients were categorized into high-risk (CHA<sub>2</sub>DS<sub>2</sub>-VASc score, >2; n = 424), moderate-risk (CHA<sub>2</sub>DS<sub>2</sub>-VASc score, 2; n = 218), and low-risk (CHA<sub>2</sub>DS<sub>2</sub>-VASc score, 0-1; n = 351) groups. The primary outcome was major adverse cardiac events (MACE) at 1 year after index AIS. Multivariate Cox regression analyses evaluated the prognostic value of CHA<sub>2</sub>DS<sub>2</sub>-VASc scores after controlling for potential confounding factors. A sensitivity analysis was performed based on 3 CHA<sub>2</sub>DS<sub>2</sub>-VASc groups generated using propensity score matching.</p><p><strong>Results: </strong>The rate of MACE during 12-month follow-up was statistically significantly higher (<i>P</i> < .01) in patients with a CHA<sub>2</sub>DS<sub>2</sub>-VASc score greater than 2 (34.7%) than in patients with a score of 2 (23.9%) or of 0 or 1 (14.8%). Multivariate Cox regression models indicated that, compared with a CHA<sub>2</sub>DS<sub>2</sub>-VASc score of 0 or 1, the hazard ratio (HR) of MACE occurrence was 3.22 (95% CI, 1.93-5.37; <i>P</i> < .01) for a CHA<sub>2</sub>DS<sub>2</sub>-VASc score greater than 2 and 1.92 (95% CI, 1.24-2.98; <i>P</i> < .01) for a CHA<sub>2</sub>DS<sub>2</sub>-VASc score of 2. When included in the Cox regression model as a continuous variable, the CHA<sub>2</sub>DS<sub>2</sub>-VASc score remained strongly associated with higher risks of MACE (HR, 1.19 [95% CI, 1.11-1.26]; <i>P</i> < .01), all-cause mortality (HR, 1.14 [95% CI, 1.05-1.23]; <i>P</i> < .01), and recurrent stroke (HR, 1.15 [95% CI, 1.06-1.256]; <i>P</i> < .01). Sensitivity analyses based on populations generated by propensity score matching yielded similar results.</p><p><strong>Conclusion: </strong>The CHA<sub>2</sub>DS<sub>2</sub>-VASc score effectively predicts MACE in patients with AIS but without AF, providing more accurate risk stratification.</p>","PeriodicalId":48680,"journal":{"name":"Texas Heart Institute Journal","volume":"52 1","pages":"e248450"},"PeriodicalIF":0.9000,"publicationDate":"2025-02-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11795280/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Texas Heart Institute Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14503/THIJ-24-8450","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Although the prognostic value of the CHA2DS2-VASc (congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, prior stroke or transient ischemic attack, vascular disease, age 65-74 years, and female sex) scoring system in patients with stroke has been explored in several studies, a research gap exists in its application, especially in patients without atrial fibrillation (AF).
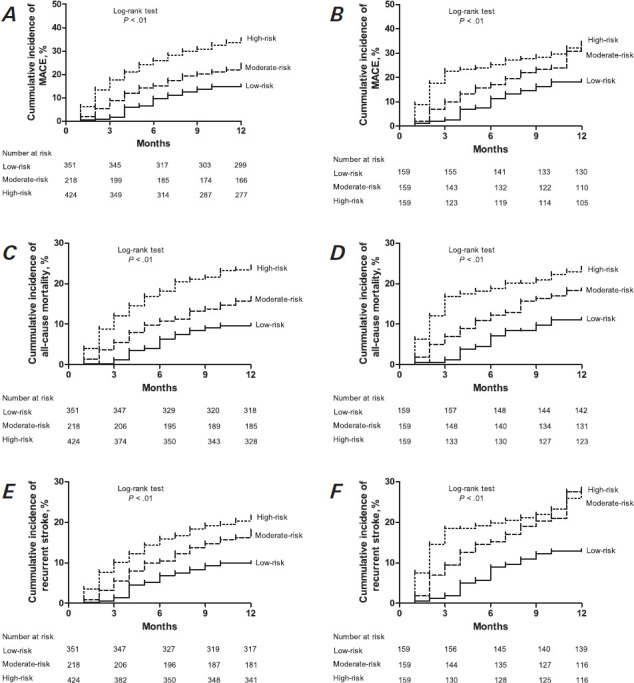
Methods: This study investigated the association between CHA2DS2-VASc score and prognosis at 1 year in patients with acute ischemic stroke (AIS) who do not have AF. A total of 993 patients with AIS but without AF were recruited between January 2019 and December 2022. Patients were categorized into high-risk (CHA2DS2-VASc score, >2; n = 424), moderate-risk (CHA2DS2-VASc score, 2; n = 218), and low-risk (CHA2DS2-VASc score, 0-1; n = 351) groups. The primary outcome was major adverse cardiac events (MACE) at 1 year after index AIS. Multivariate Cox regression analyses evaluated the prognostic value of CHA2DS2-VASc scores after controlling for potential confounding factors. A sensitivity analysis was performed based on 3 CHA2DS2-VASc groups generated using propensity score matching.
Results: The rate of MACE during 12-month follow-up was statistically significantly higher (P < .01) in patients with a CHA2DS2-VASc score greater than 2 (34.7%) than in patients with a score of 2 (23.9%) or of 0 or 1 (14.8%). Multivariate Cox regression models indicated that, compared with a CHA2DS2-VASc score of 0 or 1, the hazard ratio (HR) of MACE occurrence was 3.22 (95% CI, 1.93-5.37; P < .01) for a CHA2DS2-VASc score greater than 2 and 1.92 (95% CI, 1.24-2.98; P < .01) for a CHA2DS2-VASc score of 2. When included in the Cox regression model as a continuous variable, the CHA2DS2-VASc score remained strongly associated with higher risks of MACE (HR, 1.19 [95% CI, 1.11-1.26]; P < .01), all-cause mortality (HR, 1.14 [95% CI, 1.05-1.23]; P < .01), and recurrent stroke (HR, 1.15 [95% CI, 1.06-1.256]; P < .01). Sensitivity analyses based on populations generated by propensity score matching yielded similar results.
Conclusion: The CHA2DS2-VASc score effectively predicts MACE in patients with AIS but without AF, providing more accurate risk stratification.
期刊介绍:
For more than 45 years, the Texas Heart Institute Journal has been published by the Texas Heart Institute as part of its medical education program. Our bimonthly peer-reviewed journal enjoys a global audience of physicians, scientists, and healthcare professionals who are contributing to the prevention, diagnosis, and treatment of cardiovascular disease.
The Journal was printed under the name of Cardiovascular Diseases from 1974 through 1981 (ISSN 0093-3546). The name was changed to Texas Heart Institute Journal in 1982 and was printed through 2013 (ISSN 0730-2347). In 2014, the Journal moved to online-only publication. It is indexed by Index Medicus/MEDLINE and by other indexing and abstracting services worldwide. Our full archive is available at PubMed Central.
The Journal invites authors to submit these article types for review:
-Clinical Investigations-
Laboratory Investigations-
Reviews-
Techniques-
Coronary Anomalies-
History of Medicine-
Case Reports/Case Series (Submission Fee: $70.00 USD)-
Images in Cardiovascular Medicine (Submission Fee: $35.00 USD)-
Guest Editorials-
Peabody’s Corner-
Letters to the Editor

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


