Comparison of irinotecan/carboplatin versus etoposide/carboplatin for extended disease small cell lung cancer (ED-SCLC): A systematic review and meta-analysis of randomized controlled trials
{"title":"Comparison of irinotecan/carboplatin versus etoposide/carboplatin for extended disease small cell lung cancer (ED-SCLC): A systematic review and meta-analysis of randomized controlled trials","authors":"Zeeshan Afzal, Sara Hira, Xia Song, Na Wang","doi":"10.1002/msp2.46","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Platinum-based chemotherapy in addition to the non-platinum agent etoposide is the standard of care for extensive-stage small cell lung cancer (ES-SCLC). However, the front-line chemotherapy regimen is not known. Therefore, we aimed to perform this review comparing irinotecan/carboplatin (IC) and etoposide/carboplatin (EC) in patients of extended disease small cell lung cancer (ED-SCLC).</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We searched three databases, that is, PubMed, Embase, and Cochrane Library. The outcomes for complete response (CR), median overall survival (OS), and progression-free survival (PFS) were evaluated. In addition, adverse events such as leukopenia, thrombocytopenia, anemia, diarrhea, and infections were also assessed. RevMan 5.4.1 was used to perform the statistical analysis.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Three randomized controlled trials (RCTs) with 676 patients were included. There was a significant difference between IC and EC arms in terms of CR (risk ratio [RR] = 2.52; 95% confidence interval [CI]: 1.20−5.32; <i>p</i> = 0.02, <i>I</i><sup><i>2</i></sup> (i.e., the percentage of the total variance that is due to between-study heterogeneity) = 0%), leukopenia (RR = 0.47; 95% CI: 0.23−0.97; <i>p</i> = 0.04; <i>I</i><sup><i>2</i></sup> = 90%), amimia (RR = 0.55; 95% CI: 0.38−0.78; <i>p</i> = 0.0008; <i>I</i><sup><i>2</i></sup> = 0%), thrombocytopenia (RR = 0.51; 95% CI: 0.39–0.68; <i>p</i> = 0.00001; <i>I</i><sup><i>2</i></sup> = 0%), and diarrhea (RR = 4.88; 95% CI: 1.64−14.49; <i>p</i> = 0.004; <i>I</i><sup><i>2</i></sup> = 33%). There was no statistically significant difference between IC and EC arms in terms of median OS (hazard ratio [HR] = 1.16; 95% CI: 0.84−1.62; <i>p</i> = 0.37; <i>I</i><sup><i>2</i></sup> = 74%), PFS (HR = 1.04; 95% CI: 0.69−1.56; <i>p</i> = 0.85; <i>I</i><sup><i>2</i></sup> = 77%), nausea (RR = 1.70; 95% CI: 0.76−3.81; <i>p</i> = 0.19; <i>I</i><sup><i>2</i></sup> = 0%), infection (RR = 0.97; 95% CI: 0.64−1.48; <i>p</i> = 0.89; <i>I</i><sup><i>2</i></sup> = 0%), and treatment-related deaths (RR = 0.58; 95% CI: 0.24−1.42; <i>p</i> = 0.23; <i>I</i><sup><i>2</i></sup> = 0%).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>This meta-analysis provides valuable evidence supporting the superiority of IC regimens over EC regimens in terms of CR and toxicity profile for ED-SCLC.</p>\n </section>\n </div>","PeriodicalId":100882,"journal":{"name":"Malignancy Spectrum","volume":"1 4","pages":"300-311"},"PeriodicalIF":0.0000,"publicationDate":"2024-10-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/msp2.46","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Malignancy Spectrum","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/msp2.46","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background
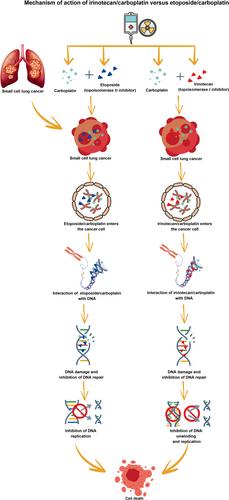
Platinum-based chemotherapy in addition to the non-platinum agent etoposide is the standard of care for extensive-stage small cell lung cancer (ES-SCLC). However, the front-line chemotherapy regimen is not known. Therefore, we aimed to perform this review comparing irinotecan/carboplatin (IC) and etoposide/carboplatin (EC) in patients of extended disease small cell lung cancer (ED-SCLC).
Methods
We searched three databases, that is, PubMed, Embase, and Cochrane Library. The outcomes for complete response (CR), median overall survival (OS), and progression-free survival (PFS) were evaluated. In addition, adverse events such as leukopenia, thrombocytopenia, anemia, diarrhea, and infections were also assessed. RevMan 5.4.1 was used to perform the statistical analysis.
Results
Three randomized controlled trials (RCTs) with 676 patients were included. There was a significant difference between IC and EC arms in terms of CR (risk ratio [RR] = 2.52; 95% confidence interval [CI]: 1.20−5.32; p = 0.02, I2 (i.e., the percentage of the total variance that is due to between-study heterogeneity) = 0%), leukopenia (RR = 0.47; 95% CI: 0.23−0.97; p = 0.04; I2 = 90%), amimia (RR = 0.55; 95% CI: 0.38−0.78; p = 0.0008; I2 = 0%), thrombocytopenia (RR = 0.51; 95% CI: 0.39–0.68; p = 0.00001; I2 = 0%), and diarrhea (RR = 4.88; 95% CI: 1.64−14.49; p = 0.004; I2 = 33%). There was no statistically significant difference between IC and EC arms in terms of median OS (hazard ratio [HR] = 1.16; 95% CI: 0.84−1.62; p = 0.37; I2 = 74%), PFS (HR = 1.04; 95% CI: 0.69−1.56; p = 0.85; I2 = 77%), nausea (RR = 1.70; 95% CI: 0.76−3.81; p = 0.19; I2 = 0%), infection (RR = 0.97; 95% CI: 0.64−1.48; p = 0.89; I2 = 0%), and treatment-related deaths (RR = 0.58; 95% CI: 0.24−1.42; p = 0.23; I2 = 0%).
Conclusion
This meta-analysis provides valuable evidence supporting the superiority of IC regimens over EC regimens in terms of CR and toxicity profile for ED-SCLC.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


