Update on the therapeutic role of metformin in the management of polycystic ovary syndrome: Effects on pathophysiologic process and fertility outcomes.
{"title":"Update on the therapeutic role of metformin in the management of polycystic ovary syndrome: Effects on pathophysiologic process and fertility outcomes.","authors":"Kerstin Mg Brand, Ulrike Gottwald-Hostalek, Aimee Andag-Silva","doi":"10.1177/17455057241311759","DOIUrl":null,"url":null,"abstract":"<p><p>Influential guidelines have supported the role of metformin in the management of polycystic ovary syndrome (PCOS) for a number of years. However, regulatory approvals for this therapeutic indication are still exceptional and exist only in a few countries, including for the originator, Glucophage®. PCOS is an insulin-resistant state, which drives hyperandrogenism and anovulatory infertility. The metabolic action of metformin involves amelioration of insulin resistance, which helps to resolve hormonal and metabolic disturbances and increases ovulation, pregnancy, and live birth rates relative to placebo. A combination of metformin with clomifene citrate (another widely used treatment for PCOS) is more effective than either alone and is a useful option in women with clomifene-resistant PCOS. Combining metformin with letrozole (1st-line agent for ovulation induction in women with PCOS and no other infertility risk factors) is not more effective than letrozole alone. Continuing metformin to the end of the 1st trimester at an effective dose (e.g. 1000-2000 mg/day) may help to reduce the rate of miscarriages. Metformin also has an adjunctive role in women with PCOS receiving assisted reproduction technology (ART) using the long gonadotrophin-releasing hormone agonist protocol, where it appears to increase the pregnancy rate and to reduce the risk of ovarian hyperstimulation syndrome. There is no role for metformin in women receiving short ART protocols. Where a successful pregnancy is achieved, metformin is generally safe for the mother and neonate. Further research is needed to define with greater precision the optimal dosage and times to initiate and discontinue metformin in women with PCOS who achieve pregnancy.</p>","PeriodicalId":75327,"journal":{"name":"Women's health (London, England)","volume":"21 ","pages":"17455057241311759"},"PeriodicalIF":2.9000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11792029/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Women's health (London, England)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/17455057241311759","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
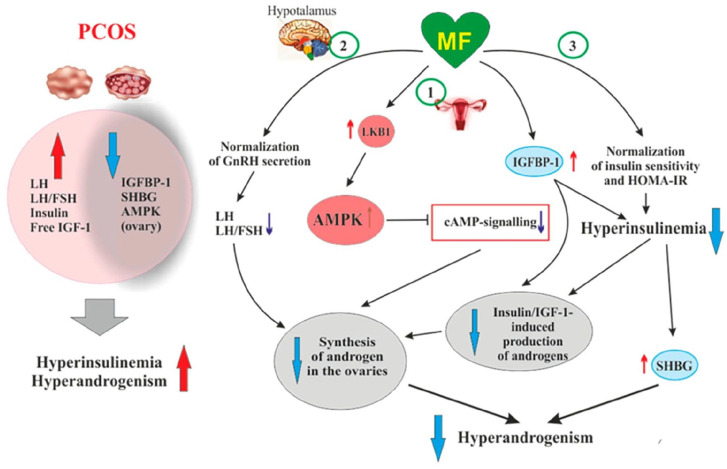
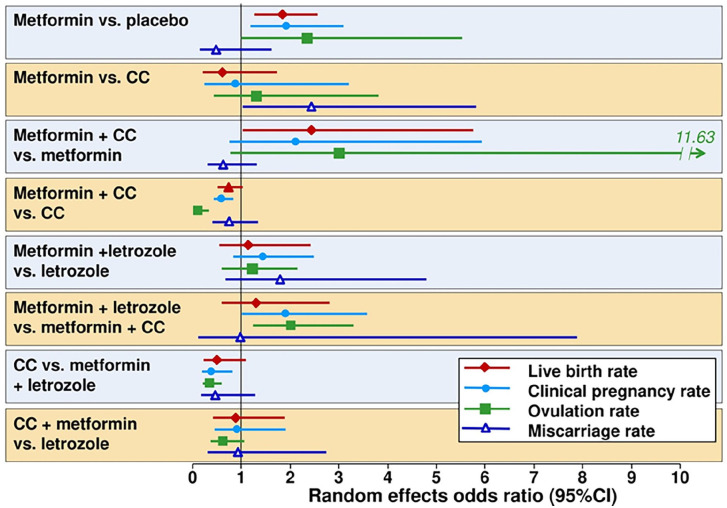
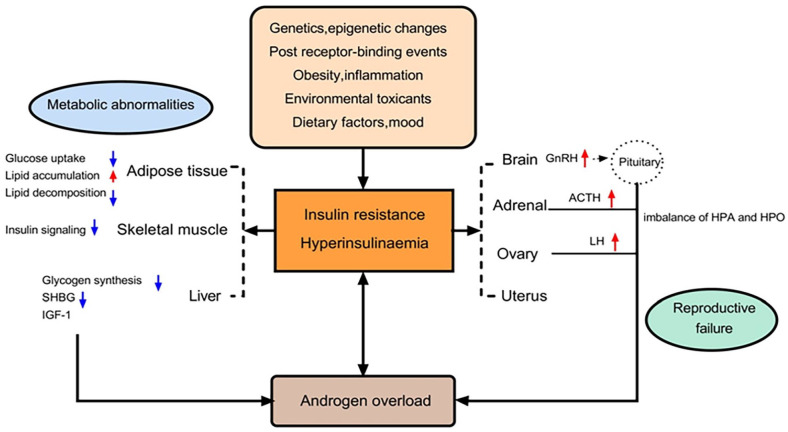
Influential guidelines have supported the role of metformin in the management of polycystic ovary syndrome (PCOS) for a number of years. However, regulatory approvals for this therapeutic indication are still exceptional and exist only in a few countries, including for the originator, Glucophage®. PCOS is an insulin-resistant state, which drives hyperandrogenism and anovulatory infertility. The metabolic action of metformin involves amelioration of insulin resistance, which helps to resolve hormonal and metabolic disturbances and increases ovulation, pregnancy, and live birth rates relative to placebo. A combination of metformin with clomifene citrate (another widely used treatment for PCOS) is more effective than either alone and is a useful option in women with clomifene-resistant PCOS. Combining metformin with letrozole (1st-line agent for ovulation induction in women with PCOS and no other infertility risk factors) is not more effective than letrozole alone. Continuing metformin to the end of the 1st trimester at an effective dose (e.g. 1000-2000 mg/day) may help to reduce the rate of miscarriages. Metformin also has an adjunctive role in women with PCOS receiving assisted reproduction technology (ART) using the long gonadotrophin-releasing hormone agonist protocol, where it appears to increase the pregnancy rate and to reduce the risk of ovarian hyperstimulation syndrome. There is no role for metformin in women receiving short ART protocols. Where a successful pregnancy is achieved, metformin is generally safe for the mother and neonate. Further research is needed to define with greater precision the optimal dosage and times to initiate and discontinue metformin in women with PCOS who achieve pregnancy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


