{"title":"Genetic background and clinical phenotype in a Vietnamese cohort with Brugada syndrome: A whole exome sequencing study.","authors":"Viet Tuan Tran, Hung Manh Pham, Phong Dinh Phan, Thinh Huy Tran, Van Khanh Tran","doi":"10.1177/20480040241310748","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The aim of this study was to report the spectrum of genetic variations and clinical phenotype in a Vietnamese cohort with confirmed Brugada syndrome (BrS) using the whole exome sequencing (WES).</p><p><strong>Methods: </strong>Fifty patients with confirmed BrS were included in this study. Genomic DNA samples were extracted from peripheral blood and conducted for WES. The variants were annotated using ANNOVAR. The variants in the 13 reported genes associated with BrS were filtered, predicted the functional impact using eight computational tools, and classified according to the 2015 ACMG guidelines.</p><p><strong>Results: </strong>Arrhythmic events were documented in one-fifth of the participants. Twenty-four probands were identified to carry 36 variants in 13 genes. Majority of the variants in our study was <i>SCN5A</i> variants (9/36 variants, 25%), followed by <i>KCNH2</i> variants (5/36 variants, 14%). The prevalence of <i>SCN5A</i> carriers was 16%; while the prevalence of minor gene carriers was less than 10%. Nine novel missense variants were identified, including four missense <i>SCN5A</i> variants (p.E901D, p.F853L, p.L377F, and p.H184R), two missense <i>ANK2</i> variants (p.S2845L and V1497L), one missense <i>CACNA1C</i> variant (M1126V), one missense <i>DSP</i> variant (p.K478N), and one intron splicing JUP variant (c.1498-5G>C).</p><p><strong>Conclusion: </strong>Our study underscores the primary significance of the <i>SCN5A</i> gene in BrS, as indicated by variant prevalence, carrier rates, pathogenicity per ACMG classification, in silico predictions, and its correlation with clinical phenotypes. Longitudinal study with larger sample size, pedigree, Sanger sequence confirmation, and functional analysis is recommended.</p>","PeriodicalId":30457,"journal":{"name":"JRSM Cardiovascular Disease","volume":"14 ","pages":"20480040241310748"},"PeriodicalIF":1.5000,"publicationDate":"2025-01-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11780628/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JRSM Cardiovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20480040241310748","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: The aim of this study was to report the spectrum of genetic variations and clinical phenotype in a Vietnamese cohort with confirmed Brugada syndrome (BrS) using the whole exome sequencing (WES).
Methods: Fifty patients with confirmed BrS were included in this study. Genomic DNA samples were extracted from peripheral blood and conducted for WES. The variants were annotated using ANNOVAR. The variants in the 13 reported genes associated with BrS were filtered, predicted the functional impact using eight computational tools, and classified according to the 2015 ACMG guidelines.
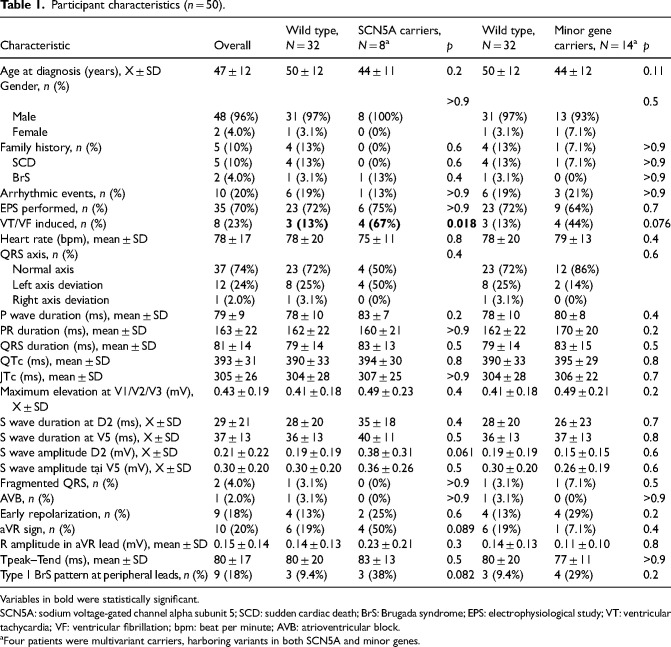
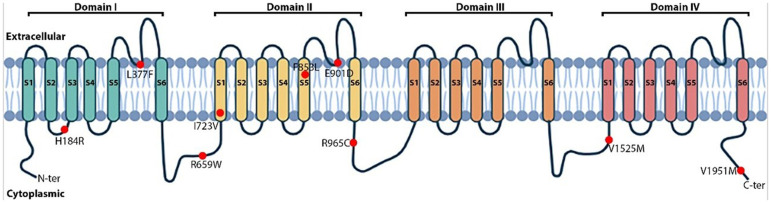
Results: Arrhythmic events were documented in one-fifth of the participants. Twenty-four probands were identified to carry 36 variants in 13 genes. Majority of the variants in our study was SCN5A variants (9/36 variants, 25%), followed by KCNH2 variants (5/36 variants, 14%). The prevalence of SCN5A carriers was 16%; while the prevalence of minor gene carriers was less than 10%. Nine novel missense variants were identified, including four missense SCN5A variants (p.E901D, p.F853L, p.L377F, and p.H184R), two missense ANK2 variants (p.S2845L and V1497L), one missense CACNA1C variant (M1126V), one missense DSP variant (p.K478N), and one intron splicing JUP variant (c.1498-5G>C).
Conclusion: Our study underscores the primary significance of the SCN5A gene in BrS, as indicated by variant prevalence, carrier rates, pathogenicity per ACMG classification, in silico predictions, and its correlation with clinical phenotypes. Longitudinal study with larger sample size, pedigree, Sanger sequence confirmation, and functional analysis is recommended.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


