Healthcare Resource Utilization Associated with Leukopenia and Neutropenia in Kidney Transplant Recipients Receiving Valganciclovir in the United States.
Qinghua Li, Vladimir Turzhitsky, Pamela Moise, Harry Jin, Kaylen Brzozowski, Irina Kolobova
{"title":"Healthcare Resource Utilization Associated with Leukopenia and Neutropenia in Kidney Transplant Recipients Receiving Valganciclovir in the United States.","authors":"Qinghua Li, Vladimir Turzhitsky, Pamela Moise, Harry Jin, Kaylen Brzozowski, Irina Kolobova","doi":"10.36469/001c.125097","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Cytomegalovirus prophylaxis in kidney transplant recipients (KTRs) is limited by post-transplant neutropenia and leukopenia (PTN/PTL). Despite its clinical significance, the healthcare resource utilization (HCRU) related to PTN/PTL remains poorly characterized. <b>Objective:</b> To evaluate HCRU among KTRs taking valganciclovir during their first year post-transplant. <b>Methods:</b> Using TriNetX Dataworks-USA, a federated, de-identified electronic medical record database, we identified adult KTRs who underwent their first kidney transplant from January 2012 to September 2020. All eligible patients were followed for 1 year. PTN/PTL was defined as absolute neutrophil count less than 1000/μL or white blood cell count less than 3500/μL. Multivariable logistic/Poisson regression models were used to assess the association between PTN/PTL and various HCRU types. <b>Results:</b> A total of 8791 KTRs were identified, of whom 6219 (70.7%) developed PTN/PTL at a mean of 5.7 months post-transplantation. Hospitalizations, rehospitalizations, emergency room visits, outpatient appointments, packed red blood cell transfusions, and granulocyte-colony stimulating factor administration were more prevalent among KTRs with PTN/PTL (61.1% vs 49.5%, 24.5% vs 14.1%, 35.2% vs 28.9%, 30.4 vs 26.2 visits, 22.3% vs 17.6%, 23.4% vs 2.2%, respectively; P < .001). Adjusted analyses confirmed that PTN/PTL correlated with increased HCRU across all categories. <b>Conclusions:</b> KTRs who developed PTN/PTL had significantly higher HCRU. Further studies are needed to evaluate strategies addressing PTN/PTL for KTRs.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"12 1","pages":"22-29"},"PeriodicalIF":2.3000,"publicationDate":"2025-01-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11784900/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36469/001c.125097","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
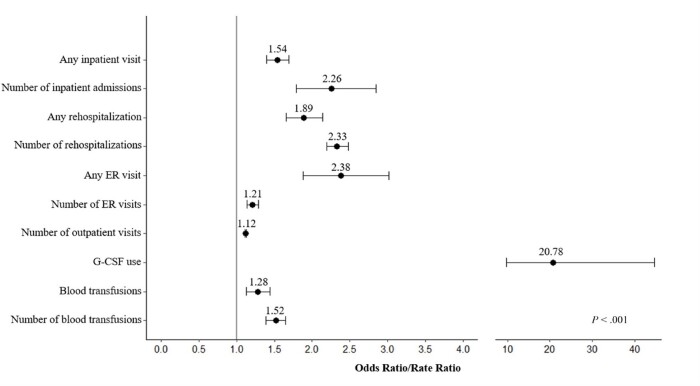
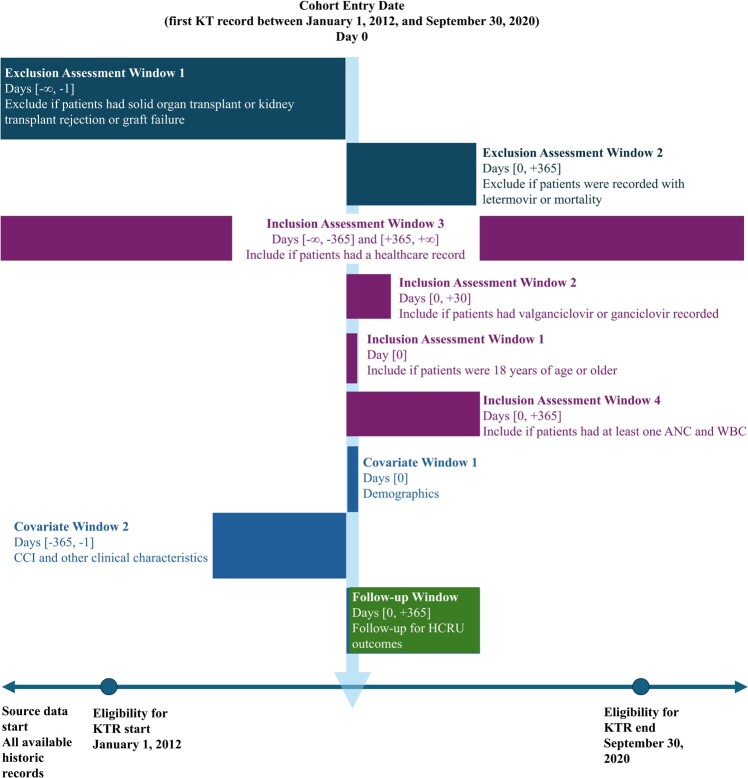
Background: Cytomegalovirus prophylaxis in kidney transplant recipients (KTRs) is limited by post-transplant neutropenia and leukopenia (PTN/PTL). Despite its clinical significance, the healthcare resource utilization (HCRU) related to PTN/PTL remains poorly characterized. Objective: To evaluate HCRU among KTRs taking valganciclovir during their first year post-transplant. Methods: Using TriNetX Dataworks-USA, a federated, de-identified electronic medical record database, we identified adult KTRs who underwent their first kidney transplant from January 2012 to September 2020. All eligible patients were followed for 1 year. PTN/PTL was defined as absolute neutrophil count less than 1000/μL or white blood cell count less than 3500/μL. Multivariable logistic/Poisson regression models were used to assess the association between PTN/PTL and various HCRU types. Results: A total of 8791 KTRs were identified, of whom 6219 (70.7%) developed PTN/PTL at a mean of 5.7 months post-transplantation. Hospitalizations, rehospitalizations, emergency room visits, outpatient appointments, packed red blood cell transfusions, and granulocyte-colony stimulating factor administration were more prevalent among KTRs with PTN/PTL (61.1% vs 49.5%, 24.5% vs 14.1%, 35.2% vs 28.9%, 30.4 vs 26.2 visits, 22.3% vs 17.6%, 23.4% vs 2.2%, respectively; P < .001). Adjusted analyses confirmed that PTN/PTL correlated with increased HCRU across all categories. Conclusions: KTRs who developed PTN/PTL had significantly higher HCRU. Further studies are needed to evaluate strategies addressing PTN/PTL for KTRs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


