{"title":"Psychosocial Determinants and Outcomes of Expedited Liver Transplant Evaluations: Insights From a Retrospective Cohort Analysis.","authors":"Katherine M Cooper, Padmavathi Srivoleti, Alessandro Colletta, Doris Tripp, Savant Mehta, Babak Movahedi, Deepika Devuni","doi":"10.1097/TXD.0000000000001745","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>As the burden of chronic liver disease and the demand for liver transplants (LT) grows, understanding the interplay between access to care and patient outcomes is increasingly important. In this study, we explored patient characteristics and transplant outcomes in patients undergoing LT evaluations, with a focus on identifying risk factors for expedited LT evaluation.</p><p><strong>Methods: </strong>This single-center retrospective cohort study included patients who underwent LT evaluation for deceased donor LT between October 2017 and July 2021. Patients were categorized by context: expedited (inpatient) and routine (outpatient) LT evaluation groups. The outcome measures included waitlist status, pre-LT mortality, and post-LT complications.</p><p><strong>Results: </strong>Of 602 patients, 26% underwent expedited LT evaluation. Patients who underwent expedited evaluation were more likely to have a history of ascites (<i>P</i> < 0.001), hepatic encephalopathy (<i>P</i> < 0.001), and spontaneous bacterial peritonitis (<i>P</i> < 0.001) and had a higher model for end-stage liver disease sodium scores (<i>P</i> < 0.001). Both mortality (35% versus 17%, <i>P</i> < 0.001) and LT (39% versus 22%, <i>P</i> < 0.001) were more common in the expedited group; post-LT mortality was similar up to 2 y. Perceived financial concerns and social security disability income were risk factors for expedited LT evaluation. In addition, greater proximity to the LT center (95% confidence interval, 1.1-6.3; <i>P</i> = 0.025) and speaking a primary language other than English (95% confidence interval, 1.0-10.7; <i>P</i> = 0.042) were risk factors for expedited LT evaluation in women but not in men.</p><p><strong>Conclusions: </strong>Expedited LT evaluations were associated with more severe illness and higher pre-LT mortality; however, post-LT outcomes were comparable with those of routine evaluations. Identifying psychosocial risk factors may enhance equity and access to LT evaluations, particularly for women who face unique challenges in this context.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"11 2","pages":"e1745"},"PeriodicalIF":1.9000,"publicationDate":"2025-01-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11781761/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001745","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
引用次数: 0
Abstract
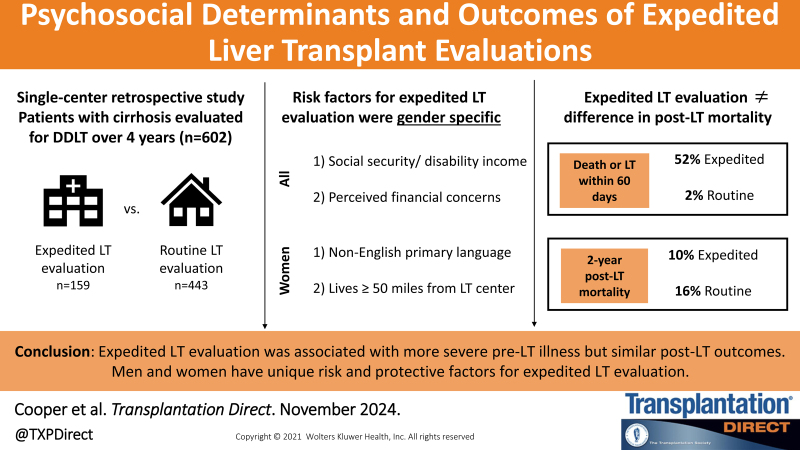
Background: As the burden of chronic liver disease and the demand for liver transplants (LT) grows, understanding the interplay between access to care and patient outcomes is increasingly important. In this study, we explored patient characteristics and transplant outcomes in patients undergoing LT evaluations, with a focus on identifying risk factors for expedited LT evaluation.
Methods: This single-center retrospective cohort study included patients who underwent LT evaluation for deceased donor LT between October 2017 and July 2021. Patients were categorized by context: expedited (inpatient) and routine (outpatient) LT evaluation groups. The outcome measures included waitlist status, pre-LT mortality, and post-LT complications.
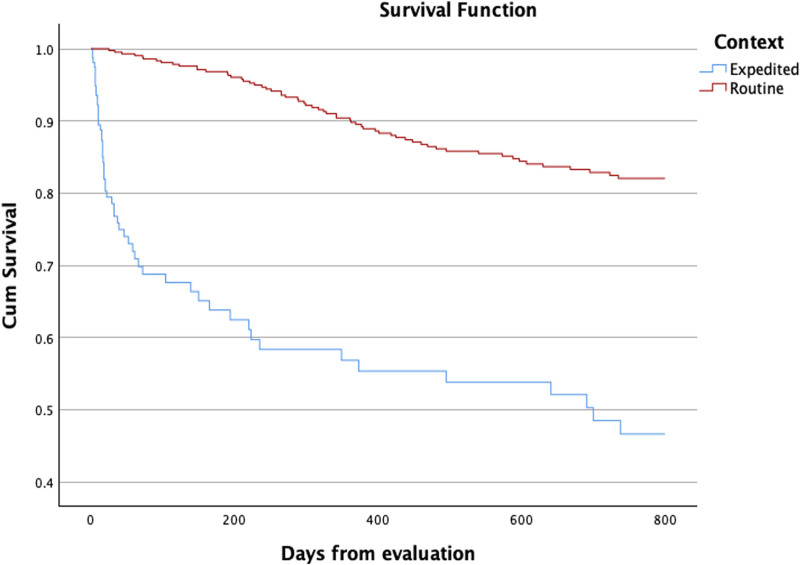
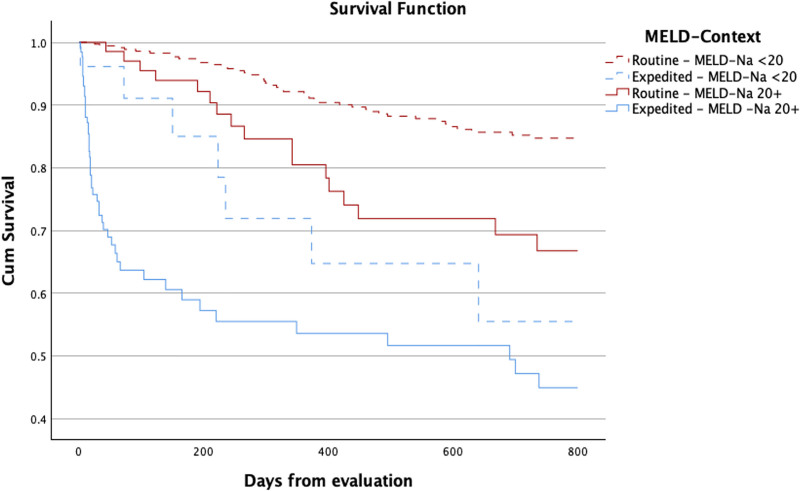
Results: Of 602 patients, 26% underwent expedited LT evaluation. Patients who underwent expedited evaluation were more likely to have a history of ascites (P < 0.001), hepatic encephalopathy (P < 0.001), and spontaneous bacterial peritonitis (P < 0.001) and had a higher model for end-stage liver disease sodium scores (P < 0.001). Both mortality (35% versus 17%, P < 0.001) and LT (39% versus 22%, P < 0.001) were more common in the expedited group; post-LT mortality was similar up to 2 y. Perceived financial concerns and social security disability income were risk factors for expedited LT evaluation. In addition, greater proximity to the LT center (95% confidence interval, 1.1-6.3; P = 0.025) and speaking a primary language other than English (95% confidence interval, 1.0-10.7; P = 0.042) were risk factors for expedited LT evaluation in women but not in men.
Conclusions: Expedited LT evaluations were associated with more severe illness and higher pre-LT mortality; however, post-LT outcomes were comparable with those of routine evaluations. Identifying psychosocial risk factors may enhance equity and access to LT evaluations, particularly for women who face unique challenges in this context.
背景:随着慢性肝病的负担和肝移植需求的增长,了解获得护理与患者预后之间的相互作用变得越来越重要。在这项研究中,我们探讨了接受肝移植评估的患者的特征和移植结果,重点是确定快速肝移植评估的危险因素。方法:这项单中心回顾性队列研究纳入了2017年10月至2021年7月期间因已故供体肝移植接受肝移植评估的患者。患者按环境分类:快速(住院)和常规(门诊)LT评估组。结果测量包括候补名单状态、肝移植前死亡率和肝移植后并发症。结果:602例患者中,26%接受了快速LT评估。接受快速评估的患者更有可能有腹水病史(P P P P P P P P = 0.025),并且主要语言不是英语(95%可信区间,1.0-10.7;P = 0.042)是女性加速LT评估的危险因素,而不是男性。结论:加速的肝移植评估与更严重的疾病和更高的肝移植前死亡率相关;然而,肝移植后的结果与常规评估相当。确定社会心理风险因素可能会提高公平和获得LT评估的机会,特别是对于在这种情况下面临独特挑战的妇女。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


