Dihydropyrimidine Dehydrogenase Deficiency (DPYD) Genotyping-Guided Fluoropyrimidine-Based Adjuvant Chemotherapy for Breast Cancer. A Cost-Effectiveness Analysis.
Dina Abushanab, Shaban Mohamed, Rania Abdel-Latif, Diala Alhaj Moustafa, Wafa Marridi, Shereen Elazzazy, Radja Badji, Wadha Al-Muftah, Said I Ismail, Salha Bujassoum, Asma Al-Thani, Daoud Al-Badriyeh, Moza Al Hail
{"title":"Dihydropyrimidine Dehydrogenase Deficiency (DPYD) Genotyping-Guided Fluoropyrimidine-Based Adjuvant Chemotherapy for Breast Cancer. A Cost-Effectiveness Analysis.","authors":"Dina Abushanab, Shaban Mohamed, Rania Abdel-Latif, Diala Alhaj Moustafa, Wafa Marridi, Shereen Elazzazy, Radja Badji, Wadha Al-Muftah, Said I Ismail, Salha Bujassoum, Asma Al-Thani, Daoud Al-Badriyeh, Moza Al Hail","doi":"10.1007/s40261-024-01413-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objective: </strong>While standard doses of adjuvant fluoropyrimidine-based chemotherapies are generally safe for most patients, the risk of severe adverse drug reactions (ADRs) is increased for those with dihydropyrimidine dehydrogenase deficiency (DPYD), a genetic variation that affects drug metabolism. The objective of this study was to examine the cost effectiveness of offering DPYD pharmacogenetic-guided care, where genetic testing informs personalized dosing versus the current standard of care (SoC), which involves administering fluoropyrimidine-based therapies without prior genetic screening, for local or metastatic breast cancer patients in Qatar.</p><p><strong>Methods: </strong>We developed a two-stage decision analysis, with an analytic tree model over a 6-month period, followed by a life-table Markov model over a lifetime horizon. We compared the current SoC with the alternate strategy of DPYD genetic screening in patients living in Qatar with local or metastatic breast cancer who were eligible for adjuvant fluoropyrimidine therapy. Clinical outcomes and utilities were obtained from published studies, while healthcare costs were estimated from Hamad Medical Corporation, Qatar. The short-term outcome included the incremental cost-effectiveness ratio (ICER), defined as cost per success (survival without grade III/IV ADRs) at 6 months. The long-term outcome was the ICER, defined as cost per quality-adjusted life year (QALY) gained, with a 3% annual discount rate. The study adopted a public healthcare perspective in Qatar. Sensitivity analyses were conducted to explore the impact of key input parameters on the robustness of the model.</p><p><strong>Results: </strong>In the short-term model, at its base case, DPYD genomic screening was dominant over SoC with a mean cost-saving of QAR84,585 (95% confidence interval [CI], 45,270-151,657). This cost saving reflects the overall economic benefits associated with the implementation of DPYD genomic screening. In the long-term model, compared to the current SoC, DPYD genetic screening would result in an ICER of QAR21,107 (95% CI -59,382-145,664) per QALY gained.</p><p><strong>Conclusion: </strong>Based on our model, implementing DPYD genetic screening to detect DPYD mutations in breast cancer patients before therapy initiation seems to be a cost-saving and cost-effective strategy in Qatar.</p>","PeriodicalId":10402,"journal":{"name":"Clinical Drug Investigation","volume":" ","pages":"151-163"},"PeriodicalIF":2.7000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11876264/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Drug Investigation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40261-024-01413-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/30 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objective: While standard doses of adjuvant fluoropyrimidine-based chemotherapies are generally safe for most patients, the risk of severe adverse drug reactions (ADRs) is increased for those with dihydropyrimidine dehydrogenase deficiency (DPYD), a genetic variation that affects drug metabolism. The objective of this study was to examine the cost effectiveness of offering DPYD pharmacogenetic-guided care, where genetic testing informs personalized dosing versus the current standard of care (SoC), which involves administering fluoropyrimidine-based therapies without prior genetic screening, for local or metastatic breast cancer patients in Qatar.
Methods: We developed a two-stage decision analysis, with an analytic tree model over a 6-month period, followed by a life-table Markov model over a lifetime horizon. We compared the current SoC with the alternate strategy of DPYD genetic screening in patients living in Qatar with local or metastatic breast cancer who were eligible for adjuvant fluoropyrimidine therapy. Clinical outcomes and utilities were obtained from published studies, while healthcare costs were estimated from Hamad Medical Corporation, Qatar. The short-term outcome included the incremental cost-effectiveness ratio (ICER), defined as cost per success (survival without grade III/IV ADRs) at 6 months. The long-term outcome was the ICER, defined as cost per quality-adjusted life year (QALY) gained, with a 3% annual discount rate. The study adopted a public healthcare perspective in Qatar. Sensitivity analyses were conducted to explore the impact of key input parameters on the robustness of the model.
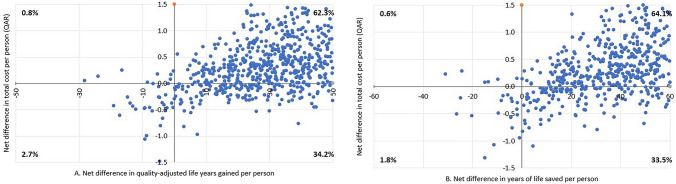
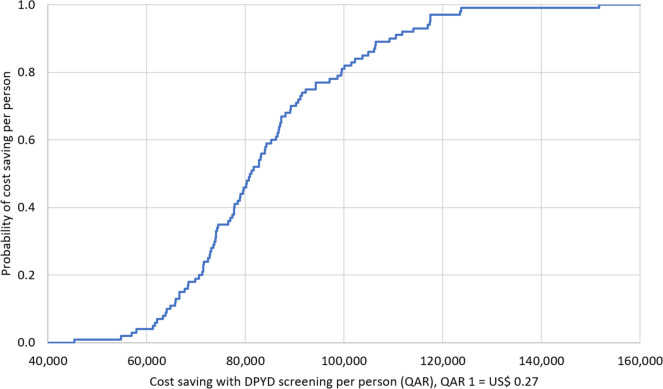
Results: In the short-term model, at its base case, DPYD genomic screening was dominant over SoC with a mean cost-saving of QAR84,585 (95% confidence interval [CI], 45,270-151,657). This cost saving reflects the overall economic benefits associated with the implementation of DPYD genomic screening. In the long-term model, compared to the current SoC, DPYD genetic screening would result in an ICER of QAR21,107 (95% CI -59,382-145,664) per QALY gained.
Conclusion: Based on our model, implementing DPYD genetic screening to detect DPYD mutations in breast cancer patients before therapy initiation seems to be a cost-saving and cost-effective strategy in Qatar.
背景和目的:虽然标准剂量的以氟嘧啶为基础的辅助化疗对大多数患者通常是安全的,但对于患有二氢嘧啶脱氢酶缺乏症(DPYD)的患者,严重药物不良反应(adr)的风险增加,这是一种影响药物代谢的遗传变异。本研究的目的是检查提供DPYD药物遗传学指导护理的成本效益,其中基因检测通知个性化剂量与目前的标准护理(SoC),其中包括在没有事先遗传筛查的情况下给予基于氟嘧啶的治疗,用于卡塔尔的局部或转移性乳腺癌患者。方法:我们开发了一个两阶段的决策分析,一个是6个月的分析树模型,然后是一个生命表马尔可夫模型。我们比较了居住在卡塔尔的局部或转移性乳腺癌患者目前的SoC和DPYD遗传筛查的替代策略,这些患者符合辅助氟嘧啶治疗的条件。临床结果和效用从已发表的研究中获得,而医疗保健费用则从卡塔尔哈马德医疗公司估计。短期结果包括6个月时的增量成本-效果比(ICER),定义为每次成功的成本(无III/IV级不良反应的生存)。长期结果是ICER,定义为每质量调整生命年(QALY)增加的成本,年贴现率为3%。该研究采用了卡塔尔公共卫生保健的观点。进行敏感性分析以探讨关键输入参数对模型鲁棒性的影响。结果:在短期模型中,在基本情况下,DPYD基因组筛查优于SoC,平均节省成本84,585卡塔尔币(95%置信区间[CI], 45,270-151,657)。这种成本节约反映了与实施DPYD基因组筛查相关的总体经济效益。在长期模型中,与当前的SoC相比,DPYD遗传筛查将导致每QALY获得的ICER为QAR21,107 (95% CI -59,382-145,664)。结论:基于我们的模型,在卡塔尔,在乳腺癌患者开始治疗前实施DPYD基因筛查检测DPYD突变似乎是一种节省成本和成本效益的策略。
期刊介绍:
Clinical Drug Investigation provides rapid publication of original research covering all phases of clinical drug development and therapeutic use of drugs. The Journal includes:
-Clinical trials, outcomes research, clinical pharmacoeconomic studies and pharmacoepidemiology studies with a strong link to optimum prescribing practice for a drug or group of drugs.
-Clinical pharmacodynamic and clinical pharmacokinetic studies with a strong link to clinical practice.
-Pharmacodynamic and pharmacokinetic studies in healthy volunteers in which significant implications for clinical prescribing are discussed.
-Studies focusing on the application of drug delivery technology in healthcare.
-Short communications and case study reports that meet the above criteria will also be considered.
Additional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in Clinical Drug Investigation may be accompanied by plain language summaries to assist readers who have some knowledge, but non in-depth expertise in, the area to understand important medical advances.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


