Diagnostic prediction model for screening of elevated low-density and non-high-density lipoproteins in young Thai adults between 20 and 40 years of age.
{"title":"Diagnostic prediction model for screening of elevated low-density and non-high-density lipoproteins in young Thai adults between 20 and 40 years of age.","authors":"Wuttipat Kiratipaisarl, Vithawat Surawattanasakul, Wachiranun Sirikul, Phichayut Phinyo","doi":"10.1136/bmjhci-2024-101180","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Low-density lipoprotein cholesterol (LDL-C) and non-high-density lipoprotein cholesterol (non-HDL-C) levels are paramount in atherosclerotic cardiovascular disease risk management. However, 94.4% of Thai young adult are unaware of their condition. A diagnostic prediction model may assist in screening and alleviating underdiagnosis.</p><p><strong>Objectives: </strong>Development and internal validation of diagnostic prediction models on elevated LDL-C (≥160 mg/dL) and non-HDL-C (≥160 mg/dL).</p><p><strong>Methods: </strong>Retrospective, single-centre, tertiary-care hospital annual health examination data from 29 March 2018 to 30 August 2023 was analysed. Two models with 11 predictors from anthropometry and bioimpedance are fitted with multivariable binary logistic regression predicting elevated LDL-C and non-HDL-C. Predictor selection used the backward stepwise elimination. Four performance metrics were quantified: discrimination using area under the receiver-operating characteristic curve (AuROC); calibration by calibration plot; utility by decision curve analysis and instability by performance instability plots. Internal validation was carried out using 500 repetitions of bootstrap-resampling.</p><p><strong>Results: </strong>Dataset included 2222 LDL-C and 5149 non-HDL-C investigations, 303 were classed as elevated LDL-C (13.6%) and 1013 as elevated non-HDL-C cases (19.7%). Two predictors, gender and metabolic age, were identified in the LDL-C model with AuROC 0.639 (95% CI 0.617 to 0.661), poor calibration, and utility in the 7%-25% probability range. Three predictors-gender, diastolic blood pressure and metabolic age-were identified in the non-HDL-C model with AuROC 0.722 (95% CI 0.705 to 0.738), good calibration and utility in 9%-55% probability range.</p><p><strong>Discussion and conclusion: </strong>Overall results demonstrated acceptable discrimination for non-HDL-C model but inadequate performance of LDL-C model for clinical practice. An external validation study should be planned for non-HDL-C model.</p>","PeriodicalId":9050,"journal":{"name":"BMJ Health & Care Informatics","volume":"32 1","pages":""},"PeriodicalIF":4.4000,"publicationDate":"2025-01-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11784327/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Health & Care Informatics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjhci-2024-101180","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Low-density lipoprotein cholesterol (LDL-C) and non-high-density lipoprotein cholesterol (non-HDL-C) levels are paramount in atherosclerotic cardiovascular disease risk management. However, 94.4% of Thai young adult are unaware of their condition. A diagnostic prediction model may assist in screening and alleviating underdiagnosis.
Objectives: Development and internal validation of diagnostic prediction models on elevated LDL-C (≥160 mg/dL) and non-HDL-C (≥160 mg/dL).
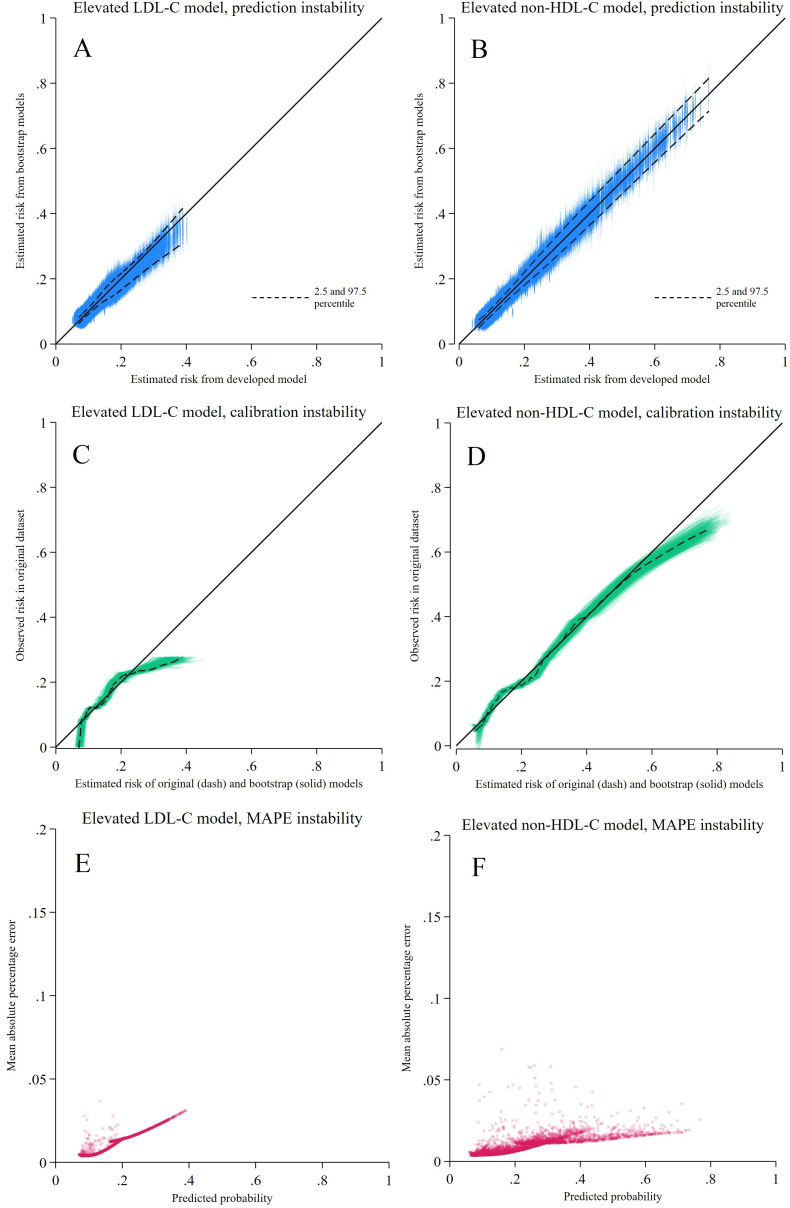
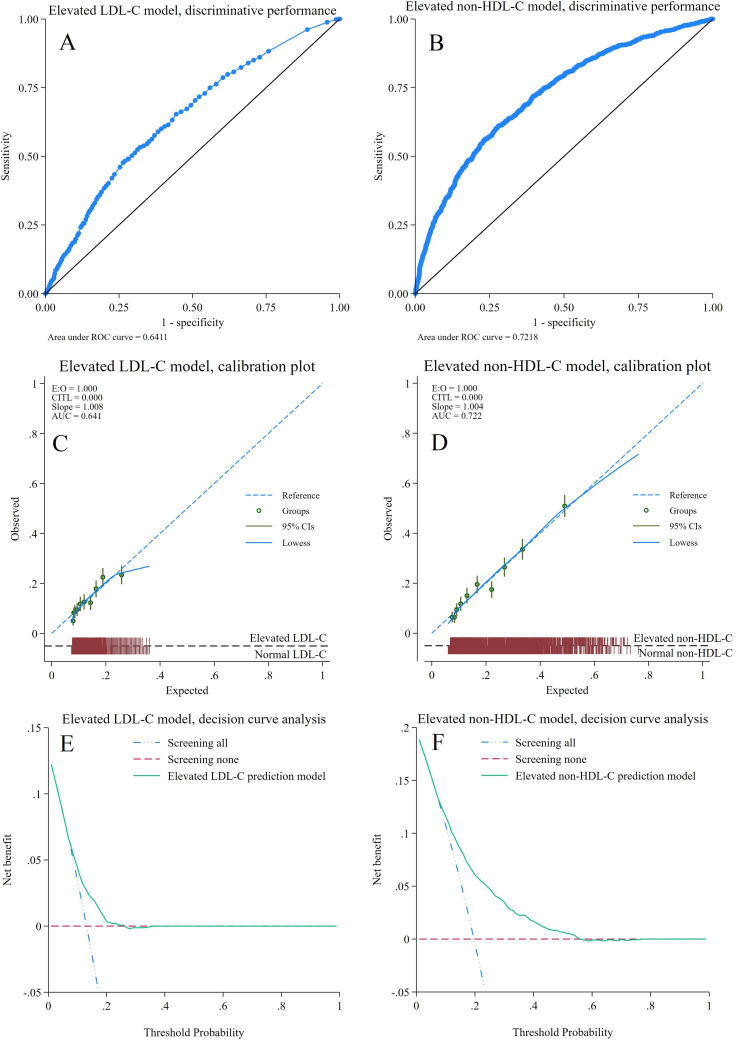
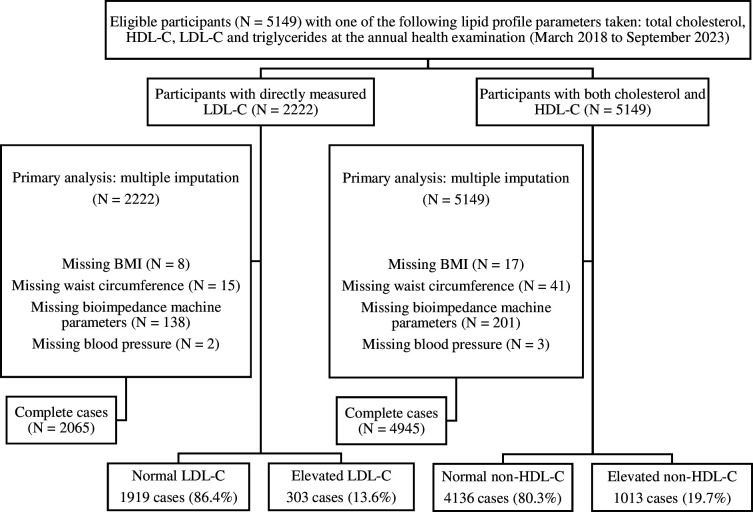
Methods: Retrospective, single-centre, tertiary-care hospital annual health examination data from 29 March 2018 to 30 August 2023 was analysed. Two models with 11 predictors from anthropometry and bioimpedance are fitted with multivariable binary logistic regression predicting elevated LDL-C and non-HDL-C. Predictor selection used the backward stepwise elimination. Four performance metrics were quantified: discrimination using area under the receiver-operating characteristic curve (AuROC); calibration by calibration plot; utility by decision curve analysis and instability by performance instability plots. Internal validation was carried out using 500 repetitions of bootstrap-resampling.
Results: Dataset included 2222 LDL-C and 5149 non-HDL-C investigations, 303 were classed as elevated LDL-C (13.6%) and 1013 as elevated non-HDL-C cases (19.7%). Two predictors, gender and metabolic age, were identified in the LDL-C model with AuROC 0.639 (95% CI 0.617 to 0.661), poor calibration, and utility in the 7%-25% probability range. Three predictors-gender, diastolic blood pressure and metabolic age-were identified in the non-HDL-C model with AuROC 0.722 (95% CI 0.705 to 0.738), good calibration and utility in 9%-55% probability range.
Discussion and conclusion: Overall results demonstrated acceptable discrimination for non-HDL-C model but inadequate performance of LDL-C model for clinical practice. An external validation study should be planned for non-HDL-C model.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


