Leila-Sophie Otten, Alessandra I G Buma, Berber Piet, Rob Ter Heine, Michel M van den Heuvel, Valesca P Retèl
{"title":"Very Early Health Technology Assessment for Potential Predictive Biomarkers in the Treatment of Advanced Non-Small Cell Lung Cancer.","authors":"Leila-Sophie Otten, Alessandra I G Buma, Berber Piet, Rob Ter Heine, Michel M van den Heuvel, Valesca P Retèl","doi":"10.1007/s41669-025-00557-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Immune checkpoint inhibitor (ICI)-containing treatment is currently prescribed as first-line treatment for all patients with advanced non-small cell lung cancer (NSCLC) without targetable driver mutations. However, only 30-45% of patients show no progression within 12 months after treatment start. Various biomarkers are being studied to save costly and potentially harmful treatment in non-responders. We evaluated the cost-effectiveness of implementing a hypothetical predictive biomarker for ICI-containing treatment response compared with standard of care (e.g., no implemented biomarker) for pembrolizumab-containing treatment in patients with advanced NSCLC in the Netherlands.</p><p><strong>Materials and methods: </strong>Standard-of-care-based and predictive-biomarker-based strategies were compared using Markov models for three first-line pembrolizumab-containing treatments depending on a patient's tumor programmed cell death ligand-1 (PD-L1) expression and histology. A Dutch healthcare system perspective was adopted. Assuming a receiver operating characteristic-area under the curve of 1.0 in identifying responders, alternative treatments were offered for non-responders in the predictive-biomarker-based strategy. Parameters and assumptions were based on real-world data from surveys, literature using a targeted search, expert opinion, and registries. Outcomes included differences in costs, survival (life years (LYs)), and survival corrected for health-related quality of life (QoL) quality-adjusted life-years (QALYs) between the predictive-biomarker- and standard-of-care-based strategy.</p><p><strong>Results: </strong>Implementing a predictive biomarker in pembrolizumab-carboplatin-paclitaxel treatment led to a mean survival reduction of 24 days (- 0.067 LYs) (18 days corrected for QoL (- 0.049 QALYs)), with cost savings of €22,606 compared with standard of care. Pembrolizumab monotherapy and pembrolizumab-pemetrexed-platinum treatments showed survival reductions of 4.5 and 3.9 months, respectively (3.6 and 2.8 months corrected for QoL), with cost savings of €24,345 and €28,456. Sensitivity analyses confirmed consistent cost savings and survival reductions. Survival losses were mainly observed due to the lower survival rates associated with the alternative first-line treatment options available for non-responders in the predictive-biomarker-based strategy within each pembrolizumab-containing treatment regimen. Pembrolizumab-carboplatin-paclitaxel treatment also showed survival gains under certain conditions related to QoL and survival estimates.</p><p><strong>Conclusions: </strong>Our study highlights the importance of careful de-implementation of ICI-treatments in advanced NSCLC, balancing costs reductions and side effects without comprising survival. In the pembrolizumab-carboplatin-paclitaxel treatment regimen, the survival loss could be considered negligible. Future research should define acceptable tradeoffs and thresholds for de-implementation, considering factors such as survival of alternative treatments and responder classification to guide predictive biomarker implementation and optimize health resource allocation.</p>","PeriodicalId":19770,"journal":{"name":"PharmacoEconomics Open","volume":" ","pages":"471-485"},"PeriodicalIF":2.1000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12037958/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PharmacoEconomics Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s41669-025-00557-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/28 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Immune checkpoint inhibitor (ICI)-containing treatment is currently prescribed as first-line treatment for all patients with advanced non-small cell lung cancer (NSCLC) without targetable driver mutations. However, only 30-45% of patients show no progression within 12 months after treatment start. Various biomarkers are being studied to save costly and potentially harmful treatment in non-responders. We evaluated the cost-effectiveness of implementing a hypothetical predictive biomarker for ICI-containing treatment response compared with standard of care (e.g., no implemented biomarker) for pembrolizumab-containing treatment in patients with advanced NSCLC in the Netherlands.
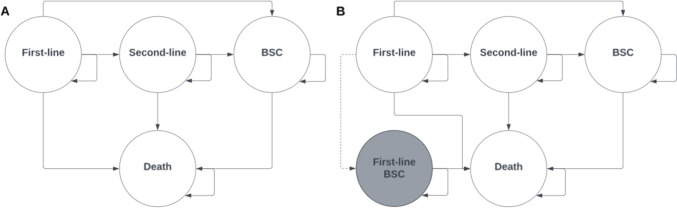
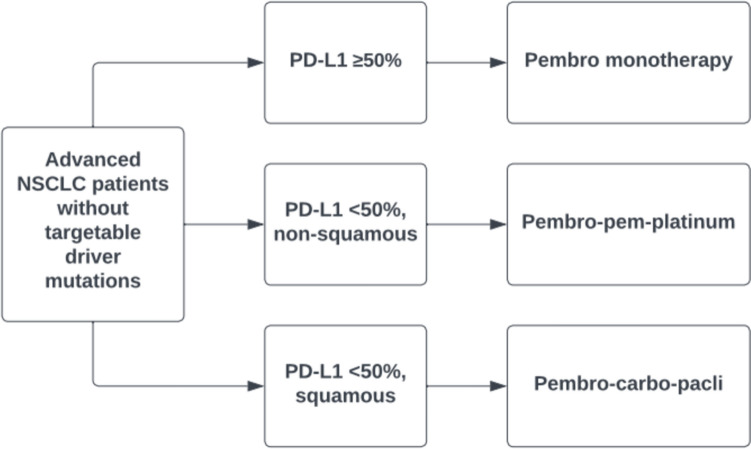
Materials and methods: Standard-of-care-based and predictive-biomarker-based strategies were compared using Markov models for three first-line pembrolizumab-containing treatments depending on a patient's tumor programmed cell death ligand-1 (PD-L1) expression and histology. A Dutch healthcare system perspective was adopted. Assuming a receiver operating characteristic-area under the curve of 1.0 in identifying responders, alternative treatments were offered for non-responders in the predictive-biomarker-based strategy. Parameters and assumptions were based on real-world data from surveys, literature using a targeted search, expert opinion, and registries. Outcomes included differences in costs, survival (life years (LYs)), and survival corrected for health-related quality of life (QoL) quality-adjusted life-years (QALYs) between the predictive-biomarker- and standard-of-care-based strategy.
Results: Implementing a predictive biomarker in pembrolizumab-carboplatin-paclitaxel treatment led to a mean survival reduction of 24 days (- 0.067 LYs) (18 days corrected for QoL (- 0.049 QALYs)), with cost savings of €22,606 compared with standard of care. Pembrolizumab monotherapy and pembrolizumab-pemetrexed-platinum treatments showed survival reductions of 4.5 and 3.9 months, respectively (3.6 and 2.8 months corrected for QoL), with cost savings of €24,345 and €28,456. Sensitivity analyses confirmed consistent cost savings and survival reductions. Survival losses were mainly observed due to the lower survival rates associated with the alternative first-line treatment options available for non-responders in the predictive-biomarker-based strategy within each pembrolizumab-containing treatment regimen. Pembrolizumab-carboplatin-paclitaxel treatment also showed survival gains under certain conditions related to QoL and survival estimates.
Conclusions: Our study highlights the importance of careful de-implementation of ICI-treatments in advanced NSCLC, balancing costs reductions and side effects without comprising survival. In the pembrolizumab-carboplatin-paclitaxel treatment regimen, the survival loss could be considered negligible. Future research should define acceptable tradeoffs and thresholds for de-implementation, considering factors such as survival of alternative treatments and responder classification to guide predictive biomarker implementation and optimize health resource allocation.
期刊介绍:
PharmacoEconomics - Open focuses on applied research on the economic implications and health outcomes associated with drugs, devices and other healthcare interventions. The journal includes, but is not limited to, the following research areas:Economic analysis of healthcare interventionsHealth outcomes researchCost-of-illness studiesQuality-of-life studiesAdditional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in PharmacoEconomics -Open may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.All manuscripts are subject to peer review by international experts. Letters to the Editor are welcomed and will be considered for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


