Neoadjuvant pyrotinib and trastuzumab in HER2-positive breast cancer with no early response (NeoPaTHer): efficacy, safety and biomarker analysis of a prospective, multicentre, response-adapted study
{"title":"Neoadjuvant pyrotinib and trastuzumab in HER2-positive breast cancer with no early response (NeoPaTHer): efficacy, safety and biomarker analysis of a prospective, multicentre, response-adapted study","authors":"Fei Wang, Yongjiu Wang, Bin Xiong, Zhenlin Yang, Jingfen Wang, Yumin Yao, Lixiang Yu, Qinye Fu, Liang Li, Qiang Zhang, Chao Zheng, Shuya Huang, Liyuan Liu, Chun Liu, Huaibo Sun, Beibei Mao, Dong-Xu Liu, Zhigang Yu","doi":"10.1038/s41392-025-02138-6","DOIUrl":null,"url":null,"abstract":"<p>The potential benefits of pyrotinib for patients with trastuzumab-insensitive, HER2-positive early-stage breast cancer remain unclear. This prospective, multicentre, response-adapted study evaluated the efficacy and safety of adding pyrotinib to the neoadjuvant treatment of HER2-positive breast cancer patients with a poor response to initial docetaxel plus carboplatin and trastuzumab (TCbH). Early response was assessed using magnetic resonance imaging (MRI) after two cycles of treatment. Patients showing poor response, as defined by RECIST 1.1, could opt to receive additional pyrotinib or continue standard therapy. The primary endpoint was the total pathological complete response (t<i>p</i>CR; ypT0/isN0) rate. Of the 129 patients enroled, 62 (48.1%) were identified as MRI-responders (cohort A), 26 non-responders continued with four more cycles of TCbH (cohort B), and 41 non-responders received additional pyrotinib (cohort C). The t<i>p</i>CR rate was 30.6% (95% CI: 20.6–43.0%) in cohort A, 15.4% (95% CI: 6.2–33.5%) in cohort B, and 29.3% (95% CI: 17.6–44.5%) in cohort C. Multivariable logistic regression analyses demonstrated comparable odds of achieving t<i>p</i>CR between cohorts A and C (odds ratio = 1.04, 95% CI: 0.40–2.70). No new adverse events were observed with the addition of pyrotinib. Patients with co-mutations of <i>TP53</i> and <i>PIK3CA</i> exhibited lower rates of early partial response compared to those without or with a single gene mutation (36.0% vs. 60.0%, <i>P</i> = 0.08). These findings suggest that adding pyrotinib may benefit patients who do not respond to neoadjuvant trastuzumab plus chemotherapy. Further investigation is warranted to identify biomarkers predicting patients’ benefit from the addition of pyrotinib.</p>","PeriodicalId":21766,"journal":{"name":"Signal Transduction and Targeted Therapy","volume":"24 1","pages":""},"PeriodicalIF":40.8000,"publicationDate":"2025-01-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Signal Transduction and Targeted Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41392-025-02138-6","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"BIOCHEMISTRY & MOLECULAR BIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
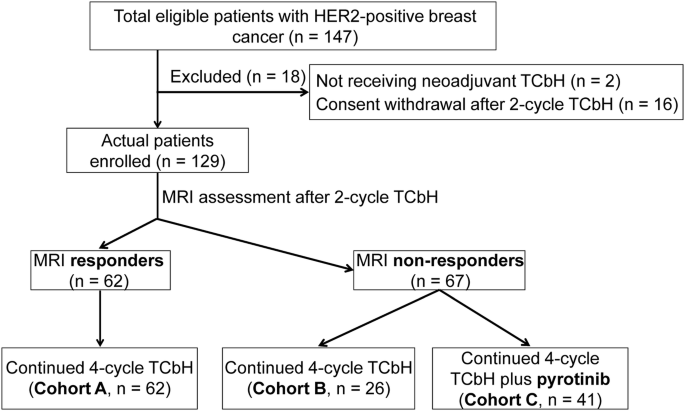
The potential benefits of pyrotinib for patients with trastuzumab-insensitive, HER2-positive early-stage breast cancer remain unclear. This prospective, multicentre, response-adapted study evaluated the efficacy and safety of adding pyrotinib to the neoadjuvant treatment of HER2-positive breast cancer patients with a poor response to initial docetaxel plus carboplatin and trastuzumab (TCbH). Early response was assessed using magnetic resonance imaging (MRI) after two cycles of treatment. Patients showing poor response, as defined by RECIST 1.1, could opt to receive additional pyrotinib or continue standard therapy. The primary endpoint was the total pathological complete response (tpCR; ypT0/isN0) rate. Of the 129 patients enroled, 62 (48.1%) were identified as MRI-responders (cohort A), 26 non-responders continued with four more cycles of TCbH (cohort B), and 41 non-responders received additional pyrotinib (cohort C). The tpCR rate was 30.6% (95% CI: 20.6–43.0%) in cohort A, 15.4% (95% CI: 6.2–33.5%) in cohort B, and 29.3% (95% CI: 17.6–44.5%) in cohort C. Multivariable logistic regression analyses demonstrated comparable odds of achieving tpCR between cohorts A and C (odds ratio = 1.04, 95% CI: 0.40–2.70). No new adverse events were observed with the addition of pyrotinib. Patients with co-mutations of TP53 and PIK3CA exhibited lower rates of early partial response compared to those without or with a single gene mutation (36.0% vs. 60.0%, P = 0.08). These findings suggest that adding pyrotinib may benefit patients who do not respond to neoadjuvant trastuzumab plus chemotherapy. Further investigation is warranted to identify biomarkers predicting patients’ benefit from the addition of pyrotinib.
期刊介绍:
Signal Transduction and Targeted Therapy is an open access journal that focuses on timely publication of cutting-edge discoveries and advancements in basic science and clinical research related to signal transduction and targeted therapy.
Scope: The journal covers research on major human diseases, including, but not limited to:
Cancer,Cardiovascular diseases,Autoimmune diseases,Nervous system diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


