Sylvain Goutelle, Olivier Bahuaud, Charlotte Genestet, Aurélien Millet, François Parant, Oana Dumitrescu, Florence Ader
{"title":"Exposure to Rifampicin and its Metabolite 25-Deacetylrifampicin Rapidly Decreases During Tuberculosis Therapy.","authors":"Sylvain Goutelle, Olivier Bahuaud, Charlotte Genestet, Aurélien Millet, François Parant, Oana Dumitrescu, Florence Ader","doi":"10.1007/s40262-025-01479-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objective: </strong>Limited information is available on the pharmacokinetics of rifampicin (RIF) along with that of its active metabolite, 25-deacetylrifampicin (25-dRIF). This study aimed to analyse the pharmacokinetic data of RIF and 25-dRIF collected in adult patients treated for tuberculosis.</p><p><strong>Methods: </strong>In adult patients receiving 10 mg/kg of RIF as part of a standard regimen for drug-susceptible pulmonary tuberculosis enrolled in the Opti-4TB study, plasma RIF and 25-dRIF concentrations were measured at various occasions. The RIF and 25-dRIF concentrations were modelled simultaneously by using a population approach. The area under the concentration-time curves of RIF and 25-dRIF were estimated on each occasion of therapeutic drug monitoring. Optimal RIF exposure, defined as an area under the concentration-time curve over 24 hours/minimum inhibitory concentration > 435, was assessed.</p><p><strong>Results: </strong>Concentration data (247 and 243 concentrations of RIF and 25-dRIF, respectively) were obtained in 35 patients with tuberculosis (10 women, 25 men). Mycobacterium tuberculosis minimum inhibitory concentration ranged from 0.06 to 0.5 mg/L (median = 0.25 mg/L). The final model was a two-compartment model including RIF metabolism into 25-dRIF and auto-induction. Exposure to 25-dRIF was low, with a mean area under the concentration-time curve over 24 h ratio of 25-dRIF/RIF of 14 ± 6%. The area under the concentration-time curve over 24 h of RIF and 25-dRIF rapidly decreased during therapy, with an auto-induction half-life of 1.6 days. Optimal RIF exposure was achieved in only six (19.3%) out of 31 patients upon first therapeutic drug monitoring.</p><p><strong>Conclusions: </strong>Exposure to both RIF and 25-dRIF rapidly decreased during tuberculosis therapy. The contribution of 25-dRIF to overall drug exposure was low. Attainment of the target area under the concentration-time curve over 24 hours/minimum inhibitory concentration for RIF was poor, supporting an increased RIF dosage as an option to compensate for auto-induction.</p>","PeriodicalId":10405,"journal":{"name":"Clinical Pharmacokinetics","volume":" ","pages":"387-396"},"PeriodicalIF":4.0000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11954713/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pharmacokinetics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40262-025-01479-3","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/27 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objective: Limited information is available on the pharmacokinetics of rifampicin (RIF) along with that of its active metabolite, 25-deacetylrifampicin (25-dRIF). This study aimed to analyse the pharmacokinetic data of RIF and 25-dRIF collected in adult patients treated for tuberculosis.
Methods: In adult patients receiving 10 mg/kg of RIF as part of a standard regimen for drug-susceptible pulmonary tuberculosis enrolled in the Opti-4TB study, plasma RIF and 25-dRIF concentrations were measured at various occasions. The RIF and 25-dRIF concentrations were modelled simultaneously by using a population approach. The area under the concentration-time curves of RIF and 25-dRIF were estimated on each occasion of therapeutic drug monitoring. Optimal RIF exposure, defined as an area under the concentration-time curve over 24 hours/minimum inhibitory concentration > 435, was assessed.
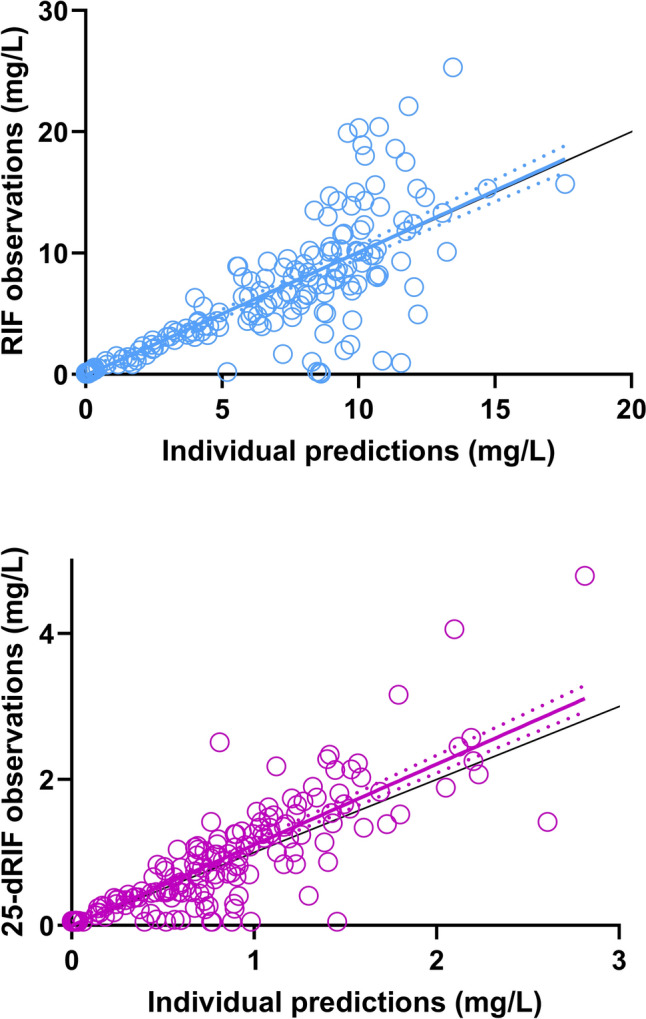
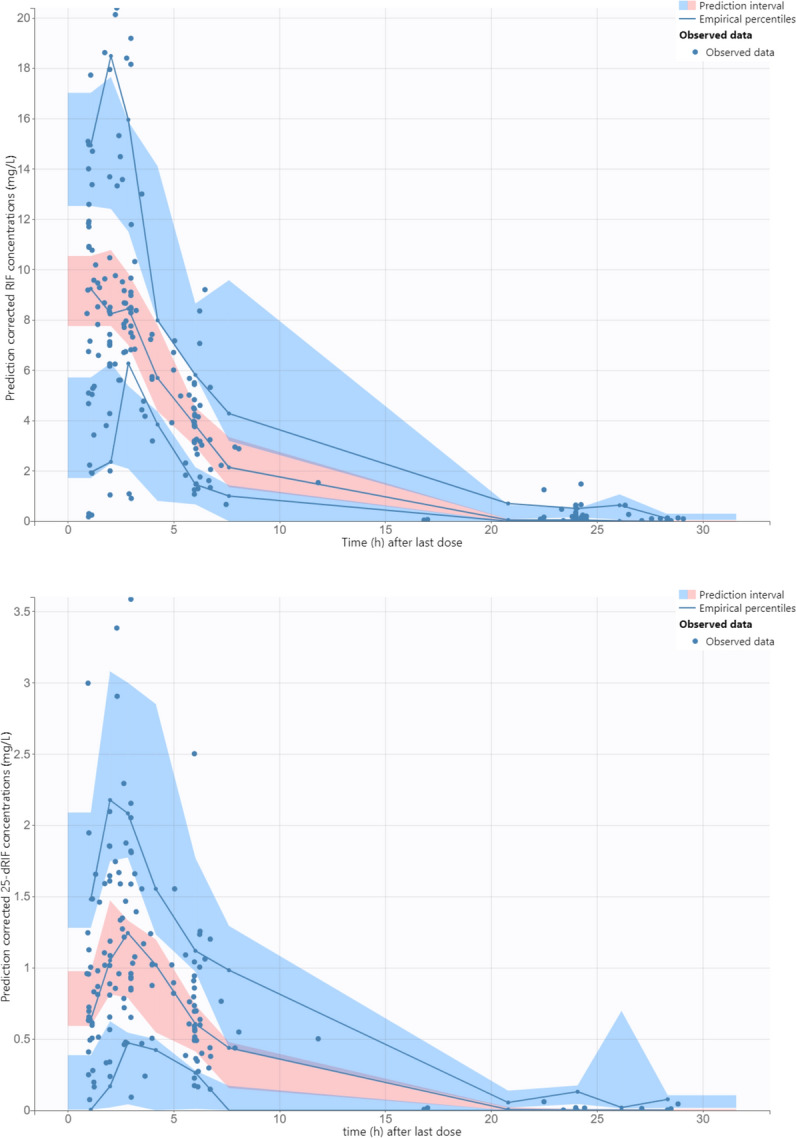
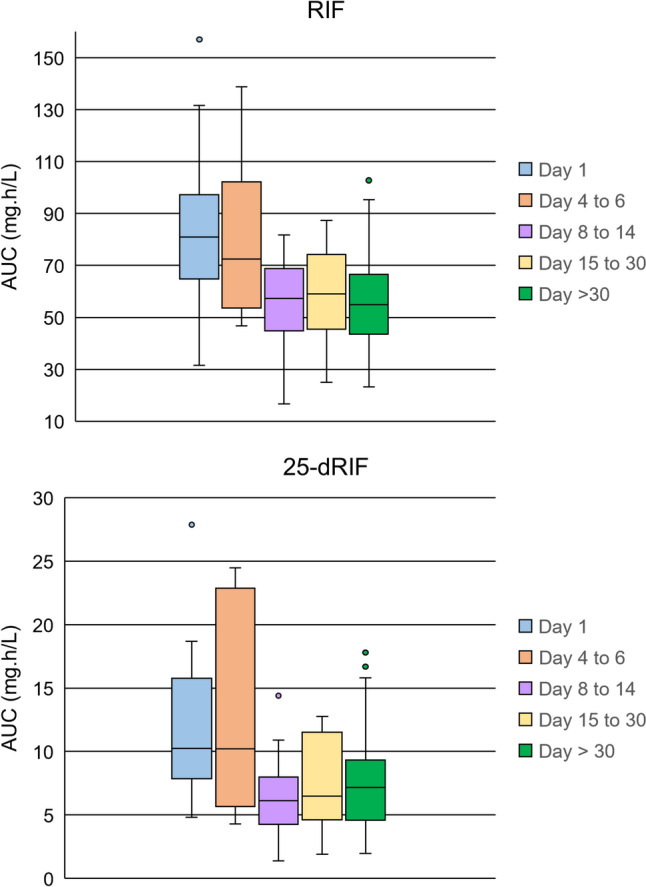
Results: Concentration data (247 and 243 concentrations of RIF and 25-dRIF, respectively) were obtained in 35 patients with tuberculosis (10 women, 25 men). Mycobacterium tuberculosis minimum inhibitory concentration ranged from 0.06 to 0.5 mg/L (median = 0.25 mg/L). The final model was a two-compartment model including RIF metabolism into 25-dRIF and auto-induction. Exposure to 25-dRIF was low, with a mean area under the concentration-time curve over 24 h ratio of 25-dRIF/RIF of 14 ± 6%. The area under the concentration-time curve over 24 h of RIF and 25-dRIF rapidly decreased during therapy, with an auto-induction half-life of 1.6 days. Optimal RIF exposure was achieved in only six (19.3%) out of 31 patients upon first therapeutic drug monitoring.
Conclusions: Exposure to both RIF and 25-dRIF rapidly decreased during tuberculosis therapy. The contribution of 25-dRIF to overall drug exposure was low. Attainment of the target area under the concentration-time curve over 24 hours/minimum inhibitory concentration for RIF was poor, supporting an increased RIF dosage as an option to compensate for auto-induction.
期刊介绍:
Clinical Pharmacokinetics promotes the continuing development of clinical pharmacokinetics and pharmacodynamics for the improvement of drug therapy, and for furthering postgraduate education in clinical pharmacology and therapeutics.
Pharmacokinetics, the study of drug disposition in the body, is an integral part of drug development and rational use. Knowledge and application of pharmacokinetic principles leads to accelerated drug development, cost effective drug use and a reduced frequency of adverse effects and drug interactions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


