Commonly prescribed medications and risk of pneumonia and all-cause mortality in people with idiopathic pulmonary fibrosis: a UK population-based cohort study.
Ann D Morgan, Georgie M Massen, Hannah R Whittaker, Iain Stewart, Gisli Jenkins, Peter M George, Jennifer K Quint
{"title":"Commonly prescribed medications and risk of pneumonia and all-cause mortality in people with idiopathic pulmonary fibrosis: a UK population-based cohort study.","authors":"Ann D Morgan, Georgie M Massen, Hannah R Whittaker, Iain Stewart, Gisli Jenkins, Peter M George, Jennifer K Quint","doi":"10.1186/s41479-024-00155-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A growing body of evidence suggests that prolonged use of inhaled corticosteroids (ICS) and proton pump inhibitors (PPIs) is associated with increased risks of pneumonia. A substantial proportion of people with idiopathic pulmonary fibrosis (IPF) are prescribed PPIs or ICS to treat common comorbidities, giving rise to concerns that use of these medications may be associated with potential harms in this patient population.</p><p><strong>Methods: </strong>We used UK Clinical Practice Research Datalink (CPRD) Aurum primary care data linked to national mortality and hospital admissions data to create a cohort of people diagnosed with IPF on or after 1 January 2010. Patients were assigned to one of three exposure categories according to their prescribing history in the 12 months prior to IPF diagnosis as follows: \"regular\" users (≥ 4 prescriptions), \"irregular\" users (1-3 prescriptions) and \"non-users\" (no prescriptions). We explored the association between PPI/ICS prescription and pneumonia hospitalisation and all-cause mortality using multinomial Cox regression models.</p><p><strong>Results: </strong>A total of 17,105 people met our study inclusion criteria; 62.6% were male and 15.9% were current smokers. Median age at IPF diagnosis was 76.7 years (IQR: 69.6-82.7). 19.9% were regularly prescribed PPIs, and 16.0% ICS, prior to IPF diagnosis. Regular prescribing of PPIs and ICS was positively associated with hospitalisation for pneumonia; the adjusted HR for pneumonia hospitalisation comparing regular PPI users with non-users was 1.14 (95%CI: 1.04-1.24); for regular ICS users the corresponding HR was 1.40 (95%CI: 1.25-1.55). We also observed a small increased risk for all-cause mortality in the \"regular ICS user\" group compared with the \"non-user\" control group (HR<sub>adj</sub> = 1.19, 1.06-1.33). We found no evidence of an association between PPI prescribing and all-cause mortality.</p><p><strong>Conclusion: </strong>Prolonged prescription of medications used to treat common comorbidities in IPF may be associated with increased risks for severe respiratory infections. These findings point to a need to adopt an adequate risk-benefit balance approach to the prescribing of ICS-containing inhalers and PPIs in people with IPF without evidence of comorbidities, especially older patients and/or those with more advanced disease in whom respiratory infections are more likely to result in poorer outcomes.</p>","PeriodicalId":45120,"journal":{"name":"Pneumonia","volume":"17 1","pages":"2"},"PeriodicalIF":6.2000,"publicationDate":"2025-01-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11762896/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pneumonia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41479-024-00155-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: A growing body of evidence suggests that prolonged use of inhaled corticosteroids (ICS) and proton pump inhibitors (PPIs) is associated with increased risks of pneumonia. A substantial proportion of people with idiopathic pulmonary fibrosis (IPF) are prescribed PPIs or ICS to treat common comorbidities, giving rise to concerns that use of these medications may be associated with potential harms in this patient population.
Methods: We used UK Clinical Practice Research Datalink (CPRD) Aurum primary care data linked to national mortality and hospital admissions data to create a cohort of people diagnosed with IPF on or after 1 January 2010. Patients were assigned to one of three exposure categories according to their prescribing history in the 12 months prior to IPF diagnosis as follows: "regular" users (≥ 4 prescriptions), "irregular" users (1-3 prescriptions) and "non-users" (no prescriptions). We explored the association between PPI/ICS prescription and pneumonia hospitalisation and all-cause mortality using multinomial Cox regression models.
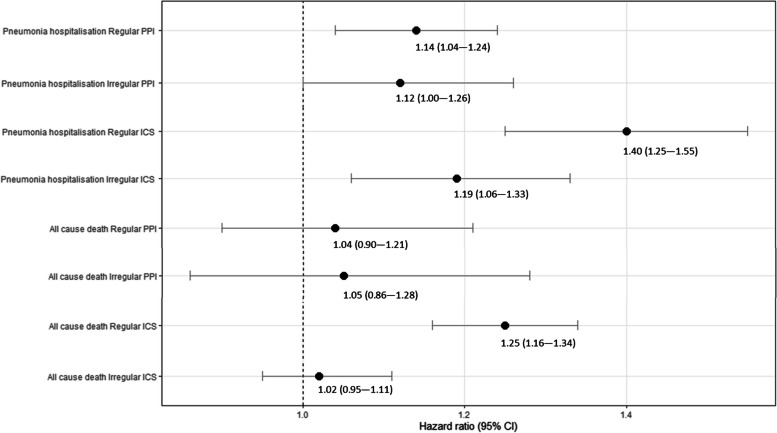
Results: A total of 17,105 people met our study inclusion criteria; 62.6% were male and 15.9% were current smokers. Median age at IPF diagnosis was 76.7 years (IQR: 69.6-82.7). 19.9% were regularly prescribed PPIs, and 16.0% ICS, prior to IPF diagnosis. Regular prescribing of PPIs and ICS was positively associated with hospitalisation for pneumonia; the adjusted HR for pneumonia hospitalisation comparing regular PPI users with non-users was 1.14 (95%CI: 1.04-1.24); for regular ICS users the corresponding HR was 1.40 (95%CI: 1.25-1.55). We also observed a small increased risk for all-cause mortality in the "regular ICS user" group compared with the "non-user" control group (HRadj = 1.19, 1.06-1.33). We found no evidence of an association between PPI prescribing and all-cause mortality.
Conclusion: Prolonged prescription of medications used to treat common comorbidities in IPF may be associated with increased risks for severe respiratory infections. These findings point to a need to adopt an adequate risk-benefit balance approach to the prescribing of ICS-containing inhalers and PPIs in people with IPF without evidence of comorbidities, especially older patients and/or those with more advanced disease in whom respiratory infections are more likely to result in poorer outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


