Role of Intraoperative Left Ventricular Global Longitudinal Strain in Hemodynamic and Cognitive Outcomes in On-Pump Coronary Artery Bypass Surgery: A Prospective Observational Study.
Eric B Lineburger, Rajesh C Arya, Celso G Junior, Fernanda S Lima, Eduardo M Búrigo, Gabriel Simoni R Fermo
{"title":"Role of Intraoperative Left Ventricular Global Longitudinal Strain in Hemodynamic and Cognitive Outcomes in On-Pump Coronary Artery Bypass Surgery: A Prospective Observational Study.","authors":"Eric B Lineburger, Rajesh C Arya, Celso G Junior, Fernanda S Lima, Eduardo M Búrigo, Gabriel Simoni R Fermo","doi":"10.4103/aca.aca_74_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The role of left ventricular global longitudinal strain (LVGLS) in coronary artery bypass grafting (CABG) and outcomes such as low cardiac output syndrome (LCOS) is not well established. The authors investigated the relationship between LVGLS before and after induction of anesthesia, their differences, and their relationship with LCOS and other outcomes.</p><p><strong>Methodology: </strong>A prospective observational study was conducted in a public/private hospital with 50 adult patients scheduled for on-pump CABG with normal left ventricular ejection fraction (LVEF). Acoustic windows necessary to obtain the 2D-LVGLS were acquired with transthoracic echocardiography (TTE) before induction of anesthesia (LVGLSBI) and after with mechanical ventilation (LVGLSAI) using transesophageal echocardiography (TEE). LCOS was defined as the use of epinephrine, dobutamine, and/or milrinone at minimum IV doses of 1 μg/min-1, 2.5 μg/kg-1/min-1, and 0.375 μg/kg-1/min-1, respectively, for a minimum of 24 h after cardiopulmonary bypass.</p><p><strong>Results: </strong>A dedicated workstation (EchoPAC Software v203, GE) was used for offline calculation of LVGLS. LVGLSBI did not have a significant correlation with LCOS (mean difference, 1.66; 95% CI, --3.63 to 3.05; P = 0.862), nevertheless, it was an independent risk factor of in-hospital mortality (OR, 0.74; 95% CI, 0.57-0.95; P = 0.02), 3-month mortality (OR, 0.80; 95% CI, 0.64-0.99; P = 0.05), and delirium (OR, 0.65; 95% CI, 0.43-0.97; P = 0.03) in the multivariate analysis. LVGLSAI was also an independent risk factor for 3-month mortality (OR, 0.78; 95% CI, 0.62-0.99; P = 0.04).</p><p><strong>Conclusions: </strong>In CABG surgeries, LVGLS was a predictor of adverse outcomes in both awake and anesthetized patients with normal LVEF.</p>","PeriodicalId":7997,"journal":{"name":"Annals of Cardiac Anaesthesia","volume":"28 1","pages":"25-32"},"PeriodicalIF":1.3000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11902346/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Cardiac Anaesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/aca.aca_74_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/20 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The role of left ventricular global longitudinal strain (LVGLS) in coronary artery bypass grafting (CABG) and outcomes such as low cardiac output syndrome (LCOS) is not well established. The authors investigated the relationship between LVGLS before and after induction of anesthesia, their differences, and their relationship with LCOS and other outcomes.
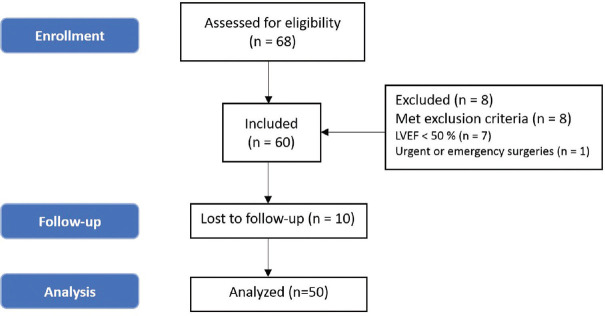
Methodology: A prospective observational study was conducted in a public/private hospital with 50 adult patients scheduled for on-pump CABG with normal left ventricular ejection fraction (LVEF). Acoustic windows necessary to obtain the 2D-LVGLS were acquired with transthoracic echocardiography (TTE) before induction of anesthesia (LVGLSBI) and after with mechanical ventilation (LVGLSAI) using transesophageal echocardiography (TEE). LCOS was defined as the use of epinephrine, dobutamine, and/or milrinone at minimum IV doses of 1 μg/min-1, 2.5 μg/kg-1/min-1, and 0.375 μg/kg-1/min-1, respectively, for a minimum of 24 h after cardiopulmonary bypass.
Results: A dedicated workstation (EchoPAC Software v203, GE) was used for offline calculation of LVGLS. LVGLSBI did not have a significant correlation with LCOS (mean difference, 1.66; 95% CI, --3.63 to 3.05; P = 0.862), nevertheless, it was an independent risk factor of in-hospital mortality (OR, 0.74; 95% CI, 0.57-0.95; P = 0.02), 3-month mortality (OR, 0.80; 95% CI, 0.64-0.99; P = 0.05), and delirium (OR, 0.65; 95% CI, 0.43-0.97; P = 0.03) in the multivariate analysis. LVGLSAI was also an independent risk factor for 3-month mortality (OR, 0.78; 95% CI, 0.62-0.99; P = 0.04).
Conclusions: In CABG surgeries, LVGLS was a predictor of adverse outcomes in both awake and anesthetized patients with normal LVEF.
期刊介绍:
Annals of Cardiac Anaesthesia (ACA) is the official journal of the Indian Association of Cardiovascular Thoracic Anaesthesiologists. The journal is indexed with PubMed/MEDLINE, Excerpta Medica/EMBASE, IndMed and MedInd. The journal’s full text is online at www.annals.in. With the aim of faster and better dissemination of knowledge, we will be publishing articles ‘Ahead of Print’ immediately on acceptance. In addition, the journal would allow free access (Open Access) to its contents, which is likely to attract more readers and citations to articles published in ACA. Authors do not have to pay for submission, processing or publication of articles in ACA.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


