Utility of Noninvasive Testing Before Invasive Coronary Angiography in the Assessment for Revascularization
Mayo Clinic proceedings. Innovations, quality & outcomes
Pub Date : 2025-02-01
DOI:10.1016/j.mayocpiqo.2024.100589
引用次数: 0
Abstract
Objective
To examine the role of noninvasive testing (NIT) before invasive coronary angiography (ICA) by evaluating the association between a positive myocardial perfusion imaging (MPI) or computed tomography angiography (CTA) result and the decision to perform coronary revascularization.
Patients and Methods
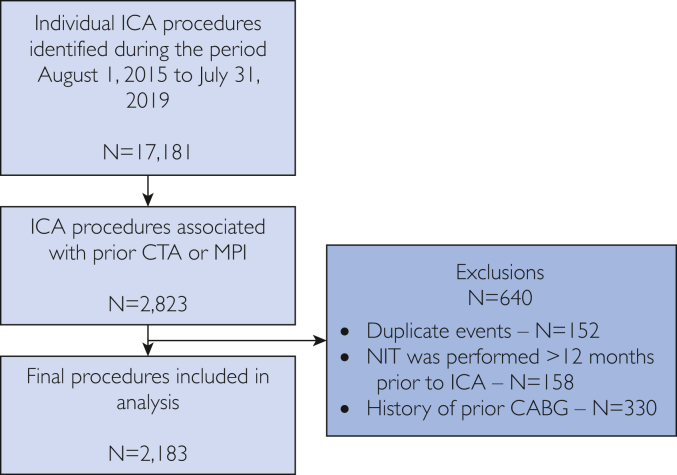
We screened all patients who received ICA between August 1, 2015, and July 31, 2019, and identified those who received MPI or CTA within the preceding 12 months. We considered MPI to be a positive result if it found moderate or severe ischemia in a specific coronary territory and CTA to be a positive result if it identified a stenosis greater than 50% in any major coronary artery.
Results
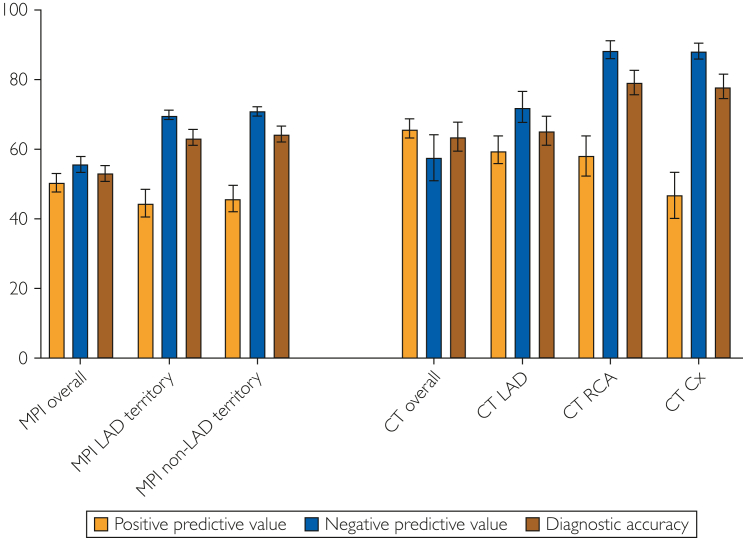
Of the 17,181 individual procedures, 2183 were included. Positive CTA had an odds ratio (OR) of 2.68 (95% CI, 1.82-3.94) for revascularization and positive MPI an OR of 1.29 (95% CI, 1.07-1.56). Overall sensitivity for CTA in the prediction of revascularization was 80.4% (95% CI, 75.7%-84.6%), with vessel-level sensitivity ranging from 57.3% (95% CI, 47.5%-66.7%) to 71.8% (95% CI, 65.8%-77.4%). Overall sensitivity of MPI was 48.2% (95% CI, 44.7%-51.7%), with territory-specific sensitivity ranging from 33.7% (95% CI, 29.9%-37.7%) to 36.5% (95% CI, 32.6%-40.6%). Overall specificity for CTA was low, at 39.5% (32.9%-46.3%), but higher when evaluating at the vessel level, ranging from 60.3% (95% CI, 54.5%-66.0%) to 83.5% (95% CI, 79.6%-86.9%). Overall specificity for MPI was 58.1% (95% CI, 54.9%-61.3%), with territory-specific specificity ranging from 78.6% (95% CI, 76.1%-80.9%) to 78.9% (95% CI, 76.5%-81.3%).
Conclusion
In this population of patients referred for ICA, positive CTA was more closely associated with revascularization than MPI. Further studies are necessary to determine the role of NIT before ICA.
有创冠状动脉造影前无创检测在血管重建评估中的应用。
目的:通过评价心肌灌注显像(MPI)或计算机断层血管造影(CTA)阳性结果与冠脉重建术决定之间的关系,探讨有创冠状动脉造影(ICA)前无创检查(NIT)的作用。患者和方法:我们筛选了2015年8月1日至2019年7月31日期间接受ICA治疗的所有患者,并确定了在过去12个月内接受MPI或CTA治疗的患者。如果MPI在特定冠状动脉区域发现中度或重度缺血,我们认为它是阳性结果;如果CTA在任何主要冠状动脉中发现狭窄大于50%,我们认为它是阳性结果。结果:在17181例单独手术中,2183例被纳入。CTA阳性血运重建术的比值比(OR)为2.68 (95% CI, 1.82-3.94), MPI阳性血运重建术的比值比(OR)为1.29 (95% CI, 1.07-1.56)。CTA预测血运重建的总体敏感性为80.4% (95% CI, 75.7%-84.6%),血管水平敏感性为57.3% (95% CI, 47.5%-66.7%)至71.8% (95% CI, 65.8%-77.4%)。MPI的总体敏感性为48.2% (95% CI, 44.7%-51.7%),区域特异性敏感性为33.7% (95% CI, 29.9%-37.7%)至36.5% (95% CI, 32.6%-40.6%)。CTA的总体特异性较低,为39.5%(32.9%-46.3%),但在血管水平评估时特异性较高,范围为60.3% (95% CI, 54.5%-66.0%)至83.5% (95% CI, 79.6%-86.9%)。MPI的总体特异性为58.1% (95% CI, 54.9%-61.3%),区域特异性范围为78.6% (95% CI, 76.1%-80.9%)至78.9% (95% CI, 76.5%-81.3%)。结论:在这群接受ICA的患者中,CTA阳性与血运重建的关系比MPI更密切。需要进一步的研究来确定NIT在ICA前的作用。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

Mayo Clinic proceedings. Innovations, quality & outcomes
Surgery, Critical Care and Intensive Care Medicine, Public Health and Health Policy
自引率
0.00%
发文量
0
审稿时长
49 days
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


