Integrating Videoconferencing Therapist Guidance Into Stepped Care Internet-Delivered Cognitive Behavioral Therapy for Child and Adolescent Anxiety: Noninferiority Randomized Controlled Trial.
Sonja March, Susan H Spence, Larry Myers, Martelle Ford, Genevieve Smith, Caroline L Donovan
{"title":"Integrating Videoconferencing Therapist Guidance Into Stepped Care Internet-Delivered Cognitive Behavioral Therapy for Child and Adolescent Anxiety: Noninferiority Randomized Controlled Trial.","authors":"Sonja March, Susan H Spence, Larry Myers, Martelle Ford, Genevieve Smith, Caroline L Donovan","doi":"10.2196/57405","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Self-guided internet-delivered cognitive behavioral therapy (ICBT) achieves greater reach than ICBT delivered with therapist guidance, but demonstrates poorer engagement and fewer clinical benefits. Alternative models of care are required that promote engagement and are effective, accessible, and scalable.</p><p><strong>Objective: </strong>This randomized trial evaluated whether a stepped care approach to ICBT using therapist guidance via videoconferencing for the step-up component (ICBT-SC[VC]) is noninferior to ICBT with full therapist delivery by videoconferencing (ICBT-TG[VC]) for child and adolescent anxiety.</p><p><strong>Methods: </strong>Participants included 137 Australian children and adolescents aged 7 to 17 years (male: n=61, 44.5%) with a primary anxiety disorder who were recruited from participants presenting to the BRAVE Online website. This noninferiority randomized trial compared ICBT-SC[VC] to an ICBT-TG[VC] program, with assessments conducted at baseline, 12 weeks, and 9 months after treatment commencement. All ICBT-TG[VC] participants received therapist guidance (videoconferencing) after each session for all 10 sessions. All ICBT-SC[VC] participants completed the first 5 sessions online without therapist guidance. If they demonstrated response to treatment after 5 sessions (defined as reductions in anxiety symptoms to the nonclinical range), they continued sessions without therapist guidance. If they did not respond, participants were stepped up to receive supplemental therapist guidance (videoconferencing) for the remaining sessions. The measures included a clinical diagnostic interview (Anxiety Disorders Interview Schedule) with clinician-rated severity rating as the primary outcome and parent- and child-reported web-based surveys assessing anxiety and anxiety-related interference (secondary outcomes).</p><p><strong>Results: </strong>Although there were no substantial differences between the treatment conditions on primary and most secondary outcome measures, the noninferiority of ICBT-SC[VC] compared to ICBT-TG[VC] could not be determined. Significant clinical benefits were evident for participants in both treatments, although this was significantly higher for the ICBT-TG[VC] participants. Of the 89 participants (38 in ICBT-SC[VC] and 51 in ICBT-TG[VC]) who remained in the study, 26 (68%) in ICBT-SC[VC] and 45 (88%) in ICBT-TG[VC] were free of their primary anxiety diagnosis by the 9-month follow-up. For the intention-to-treat sample (N=137), 41% (27/66) ICBT-SC[VC], and 69% (49/71) ICBT-TG[VC] participants were free of their primary anxiety diagnosis. Therapy compliance was lower for the ICBT-SC[VC] participants (mean 7.39, SD 3.44 sessions) than for the ICBT-TG[VC] participants (mean 8.73, SD 3.08 sessions), although treatment satisfaction was moderate to high in both conditions.</p><p><strong>Conclusions: </strong>This study provided further support for the benefits of low-intensity ICBT for children and adolescents with a primary anxiety disorder and highlighted the excellent treatment outcomes that can be achieved through therapist-guided ICBT delivered via videoconferencing. Although noninferiority of the stepped care adaptive approach could not be determined, it was acceptable to families, produced good outcomes, and could assist in increasing access to evidence-based care.</p><p><strong>Trial registration: </strong>Australian New Zealand Clinical Trials Registry (ANZCTR) ACTRN12618001418268; https://anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12618001418268.</p>","PeriodicalId":48616,"journal":{"name":"Jmir Mental Health","volume":"12 ","pages":"e57405"},"PeriodicalIF":5.8000,"publicationDate":"2025-01-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11799812/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Jmir Mental Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2196/57405","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PSYCHIATRY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Self-guided internet-delivered cognitive behavioral therapy (ICBT) achieves greater reach than ICBT delivered with therapist guidance, but demonstrates poorer engagement and fewer clinical benefits. Alternative models of care are required that promote engagement and are effective, accessible, and scalable.
Objective: This randomized trial evaluated whether a stepped care approach to ICBT using therapist guidance via videoconferencing for the step-up component (ICBT-SC[VC]) is noninferior to ICBT with full therapist delivery by videoconferencing (ICBT-TG[VC]) for child and adolescent anxiety.
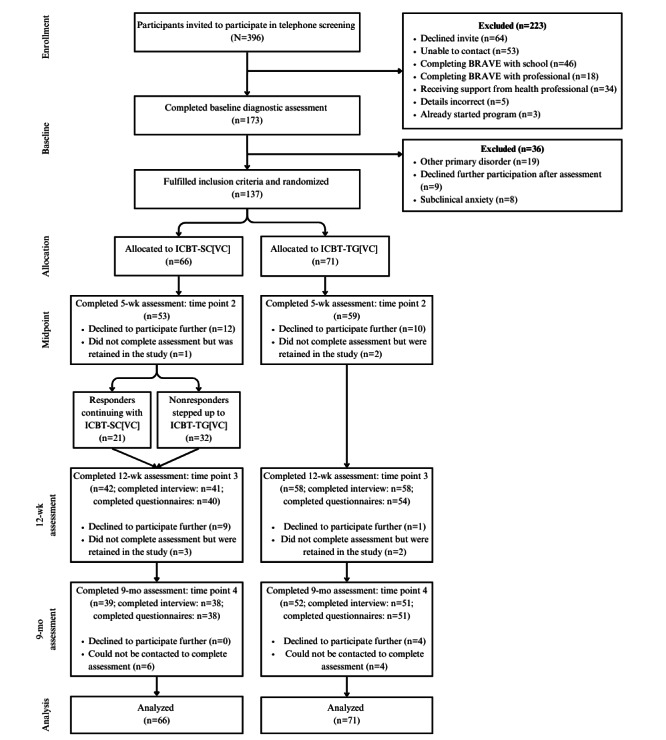
Methods: Participants included 137 Australian children and adolescents aged 7 to 17 years (male: n=61, 44.5%) with a primary anxiety disorder who were recruited from participants presenting to the BRAVE Online website. This noninferiority randomized trial compared ICBT-SC[VC] to an ICBT-TG[VC] program, with assessments conducted at baseline, 12 weeks, and 9 months after treatment commencement. All ICBT-TG[VC] participants received therapist guidance (videoconferencing) after each session for all 10 sessions. All ICBT-SC[VC] participants completed the first 5 sessions online without therapist guidance. If they demonstrated response to treatment after 5 sessions (defined as reductions in anxiety symptoms to the nonclinical range), they continued sessions without therapist guidance. If they did not respond, participants were stepped up to receive supplemental therapist guidance (videoconferencing) for the remaining sessions. The measures included a clinical diagnostic interview (Anxiety Disorders Interview Schedule) with clinician-rated severity rating as the primary outcome and parent- and child-reported web-based surveys assessing anxiety and anxiety-related interference (secondary outcomes).
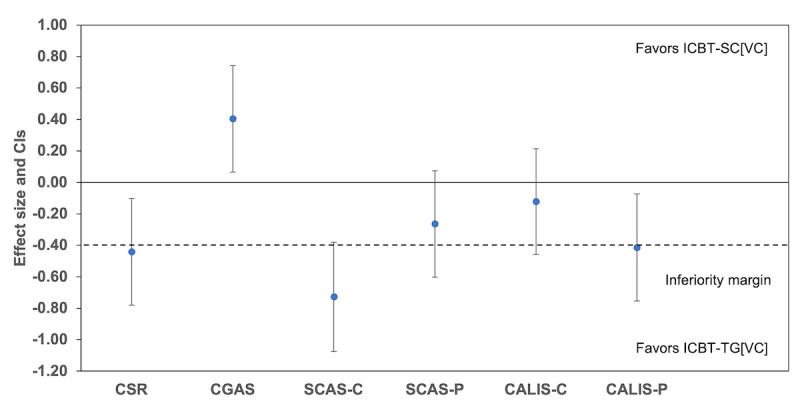
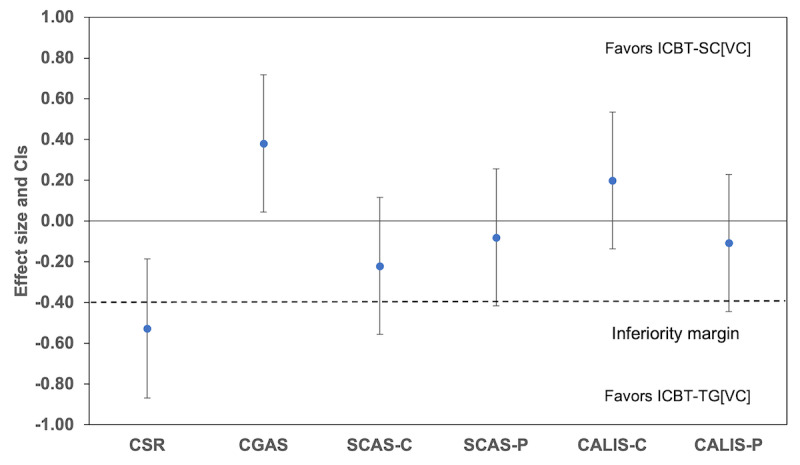
Results: Although there were no substantial differences between the treatment conditions on primary and most secondary outcome measures, the noninferiority of ICBT-SC[VC] compared to ICBT-TG[VC] could not be determined. Significant clinical benefits were evident for participants in both treatments, although this was significantly higher for the ICBT-TG[VC] participants. Of the 89 participants (38 in ICBT-SC[VC] and 51 in ICBT-TG[VC]) who remained in the study, 26 (68%) in ICBT-SC[VC] and 45 (88%) in ICBT-TG[VC] were free of their primary anxiety diagnosis by the 9-month follow-up. For the intention-to-treat sample (N=137), 41% (27/66) ICBT-SC[VC], and 69% (49/71) ICBT-TG[VC] participants were free of their primary anxiety diagnosis. Therapy compliance was lower for the ICBT-SC[VC] participants (mean 7.39, SD 3.44 sessions) than for the ICBT-TG[VC] participants (mean 8.73, SD 3.08 sessions), although treatment satisfaction was moderate to high in both conditions.
Conclusions: This study provided further support for the benefits of low-intensity ICBT for children and adolescents with a primary anxiety disorder and highlighted the excellent treatment outcomes that can be achieved through therapist-guided ICBT delivered via videoconferencing. Although noninferiority of the stepped care adaptive approach could not be determined, it was acceptable to families, produced good outcomes, and could assist in increasing access to evidence-based care.
Trial registration: Australian New Zealand Clinical Trials Registry (ANZCTR) ACTRN12618001418268; https://anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12618001418268.
期刊介绍:
JMIR Mental Health (JMH, ISSN 2368-7959) is a PubMed-indexed, peer-reviewed sister journal of JMIR, the leading eHealth journal (Impact Factor 2016: 5.175).
JMIR Mental Health focusses on digital health and Internet interventions, technologies and electronic innovations (software and hardware) for mental health, addictions, online counselling and behaviour change. This includes formative evaluation and system descriptions, theoretical papers, review papers, viewpoint/vision papers, and rigorous evaluations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


