{"title":"Oral dydrogesterone versus oral micronized progesterone in threatened miscarriage: protocol paper for a randomized controlled trial.","authors":"Alka Kriplani, Gouri Shankar Kamilya, T Ramani Devi, Ashima Taneja, Amol Pawar, Gayathri Karthik Nagesh, Tapan Pattanaik, Tanusree Gupta, Mahima Jain, Monjori Mitra","doi":"10.1530/RAF-24-0044","DOIUrl":null,"url":null,"abstract":"<p><strong>Graphical abstract: </strong></p><p><strong>Abstract: </strong>Threatened miscarriage is a common complication of early pregnancy characterized by symptoms of vaginal bleeding with/without abdominal cramps/pain in the first trimester. Progestogens are often administered for the management of this condition. Presented herein is the protocol of an ongoing, multicentric clinical trial to investigate the efficacy and safety of micronized progesterone (natural progestogen) compared to dydrogesterone (synthetic isomer of progesterone). A total of 304 eligible pregnant women aged 20-39 years, diagnosed with threatened miscarriage, will be enrolled during 5-12 weeks of gestation and randomized equally to receive either oral dydrogesterone (40 mg stat, followed by 10 mg three times a day) or oral micronized progesterone (200 mg two times a day) up to one week after stoppage of bleeding or if bleeding does not stop, then treatment will be continued till a maximum of 14 weeks of gestation (unless miscarriage is confirmed earlier or the investigator decides to prolong treatment for better outcome or if bleeding relapses). Scheduled visits after enrollment will be conducted during 6-13, 8-14, 18-20 and 24-26 weeks of gestation, in addition to a visit at the end of treatment at 14 weeks and another after parturition. The primary endpoint of the study is the miscarriage rate before 20 weeks of gestation. Secondary endpoints include the ongoing pregnancy rate at 24 weeks, treatment-induced changes in serum levels of cytokines and time to symptom resolution. Apart from the incidence of treatment-emergent adverse events, safety endpoints include changes in complete blood count and the results of liver and kidney function tests from baseline to 14 and 24-26 weeks of gestation. Delivery outcomes are exploratory endpoints of the study.</p><p><strong>Lay summary: </strong>Almost one out of four women face miscarriage during the first trimester of pregnancy; initial symptoms include vaginal bleeding with/without abdominal cramps/pain. This paper presents the plan of how an ongoing, multicentric study will be conducted to compare the efficacy and safety of oral medications known to reduce chances of miscarriage: micronized progesterone (which is a natural female sex hormone) versus synthetic progesterone. Women aged 20-39 years who are at risk of miscarriage during the first trimester of pregnancy will be randomly treated with either medication till one week after stoppage of bleeding during early pregnancy. If bleeding does not stop, treatment will be continued till a maximum of 14 weeks of pregnancy (unless miscarriage is confirmed earlier). The participants will be monitored until delivery. The study will evaluate the proportion of participants who experience miscarriage before 20 weeks of pregnancy and those who have an ongoing pregnancy at 24 weeks. It will also look at the time taken for relief from symptoms such as vaginal bleeding and abdominal pain, outcomes of delivery and incidence of any untoward event. In addition to routine tests and scans, additional tests will check for levels of biochemical parameters in the body, which are regulated by the natural or synthetic progesterone.</p><p><strong>Clinical trial registration number: </strong>CTRI/2024/02/063174 [Registered on: 26/02/2024].</p>","PeriodicalId":101312,"journal":{"name":"Reproduction & fertility","volume":" ","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2025-02-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11825165/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Reproduction & fertility","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/RAF-24-0044","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"Print","JCR":"Q2","JCRName":"REPRODUCTIVE BIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Graphical abstract:
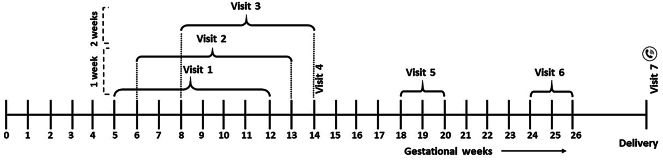
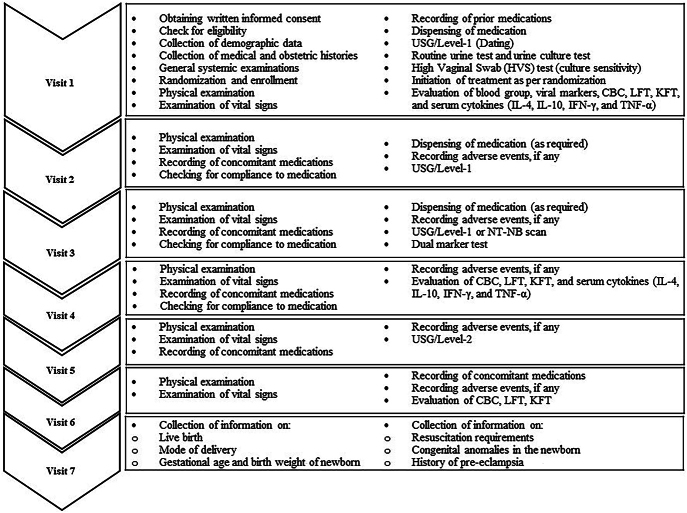
Abstract: Threatened miscarriage is a common complication of early pregnancy characterized by symptoms of vaginal bleeding with/without abdominal cramps/pain in the first trimester. Progestogens are often administered for the management of this condition. Presented herein is the protocol of an ongoing, multicentric clinical trial to investigate the efficacy and safety of micronized progesterone (natural progestogen) compared to dydrogesterone (synthetic isomer of progesterone). A total of 304 eligible pregnant women aged 20-39 years, diagnosed with threatened miscarriage, will be enrolled during 5-12 weeks of gestation and randomized equally to receive either oral dydrogesterone (40 mg stat, followed by 10 mg three times a day) or oral micronized progesterone (200 mg two times a day) up to one week after stoppage of bleeding or if bleeding does not stop, then treatment will be continued till a maximum of 14 weeks of gestation (unless miscarriage is confirmed earlier or the investigator decides to prolong treatment for better outcome or if bleeding relapses). Scheduled visits after enrollment will be conducted during 6-13, 8-14, 18-20 and 24-26 weeks of gestation, in addition to a visit at the end of treatment at 14 weeks and another after parturition. The primary endpoint of the study is the miscarriage rate before 20 weeks of gestation. Secondary endpoints include the ongoing pregnancy rate at 24 weeks, treatment-induced changes in serum levels of cytokines and time to symptom resolution. Apart from the incidence of treatment-emergent adverse events, safety endpoints include changes in complete blood count and the results of liver and kidney function tests from baseline to 14 and 24-26 weeks of gestation. Delivery outcomes are exploratory endpoints of the study.
Lay summary: Almost one out of four women face miscarriage during the first trimester of pregnancy; initial symptoms include vaginal bleeding with/without abdominal cramps/pain. This paper presents the plan of how an ongoing, multicentric study will be conducted to compare the efficacy and safety of oral medications known to reduce chances of miscarriage: micronized progesterone (which is a natural female sex hormone) versus synthetic progesterone. Women aged 20-39 years who are at risk of miscarriage during the first trimester of pregnancy will be randomly treated with either medication till one week after stoppage of bleeding during early pregnancy. If bleeding does not stop, treatment will be continued till a maximum of 14 weeks of pregnancy (unless miscarriage is confirmed earlier). The participants will be monitored until delivery. The study will evaluate the proportion of participants who experience miscarriage before 20 weeks of pregnancy and those who have an ongoing pregnancy at 24 weeks. It will also look at the time taken for relief from symptoms such as vaginal bleeding and abdominal pain, outcomes of delivery and incidence of any untoward event. In addition to routine tests and scans, additional tests will check for levels of biochemical parameters in the body, which are regulated by the natural or synthetic progesterone.
Clinical trial registration number: CTRI/2024/02/063174 [Registered on: 26/02/2024].


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


