Nowcasting to Monitor Real-Time Mpox Trends During the 2022 Outbreak in New York City: Evaluation Using Reportable Disease Data Stratified by Race or Ethnicity.
Rebecca Rohrer, Allegra Wilson, Jennifer Baumgartner, Nicole Burton, Ray R Ortiz, Alan Dorsinville, Lucretia E Jones, Sharon K Greene
{"title":"Nowcasting to Monitor Real-Time Mpox Trends During the 2022 Outbreak in New York City: Evaluation Using Reportable Disease Data Stratified by Race or Ethnicity.","authors":"Rebecca Rohrer, Allegra Wilson, Jennifer Baumgartner, Nicole Burton, Ray R Ortiz, Alan Dorsinville, Lucretia E Jones, Sharon K Greene","doi":"10.2196/56495","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Applying nowcasting methods to partially accrued reportable disease data can help policymakers interpret recent epidemic trends despite data lags and quickly identify and remediate health inequities. During the 2022 mpox outbreak in New York City, we applied Nowcasting by Bayesian Smoothing (NobBS) to estimate recent cases, citywide and stratified by race or ethnicity (Black or African American, Hispanic or Latino, and White). However, in real time, it was unclear if the estimates were accurate.</p><p><strong>Objective: </strong>We evaluated the accuracy of estimated mpox case counts across a range of NobBS implementation options.</p><p><strong>Methods: </strong>We evaluated NobBS performance for New York City residents with a confirmed or probable mpox diagnosis or illness onset from July 8 through September 30, 2022, as compared with fully accrued cases. We used the exponentiated average log score (average score) to compare moving window lengths, stratifying or not by race or ethnicity, diagnosis and onset dates, and daily and weekly aggregation.</p><p><strong>Results: </strong>During the study period, 3305 New York City residents were diagnosed with mpox (median 4, IQR 3-5 days from diagnosis to diagnosis report). Of these, 812 (25%) had missing onset dates, and of these, 230 (28%) had unknown race or ethnicity. The median lag in days from onset to onset report was 10 (IQR 7-14). For daily hindcasts by diagnosis date, the average score was 0.27 for the 14-day moving window used in real time. Average scores improved (increased) with longer moving windows (maximum: 0.47 for 49-day window). Stratifying by race or ethnicity improved performance, with an overall average score of 0.38 for the 14-day moving window (maximum: 0.57 for 49 day-window). Hindcasts for White patients performed best, with average scores of 0.45 for the 14-day window and 0.75 for the 49-day window. For unstratified, daily hindcasts by onset date, the average score ranged from 0.16 for the 42-day window to 0.30 for the 14-day window. Performance was not improved by weekly aggregation. Hindcasts underestimated diagnoses in early August after the epidemic peaked, then overestimated diagnoses in late August as the epidemic waned. Estimates were most accurate during September when cases were low and stable.</p><p><strong>Conclusions: </strong>Performance was better when hindcasting by diagnosis date than by onset date, consistent with shorter lags and higher completeness for diagnoses. For daily hindcasts by diagnosis date, longer moving windows performed better, but direct comparisons are limited because longer windows could only be assessed after case counts in this outbreak had stabilized. Stratification by race or ethnicity improved performance and identified differences in epidemic trends across patient groups. Contributors to differences in performance across strata might include differences in case volume, epidemic trends, delay distributions, and interview success rates. Health departments need reliable nowcasting and rapid evaluation tools, particularly to promote health equity by ensuring accurate estimates within all strata.</p>","PeriodicalId":74345,"journal":{"name":"Online journal of public health informatics","volume":"17 ","pages":"e56495"},"PeriodicalIF":1.1000,"publicationDate":"2025-01-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11750114/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Online journal of public health informatics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/56495","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
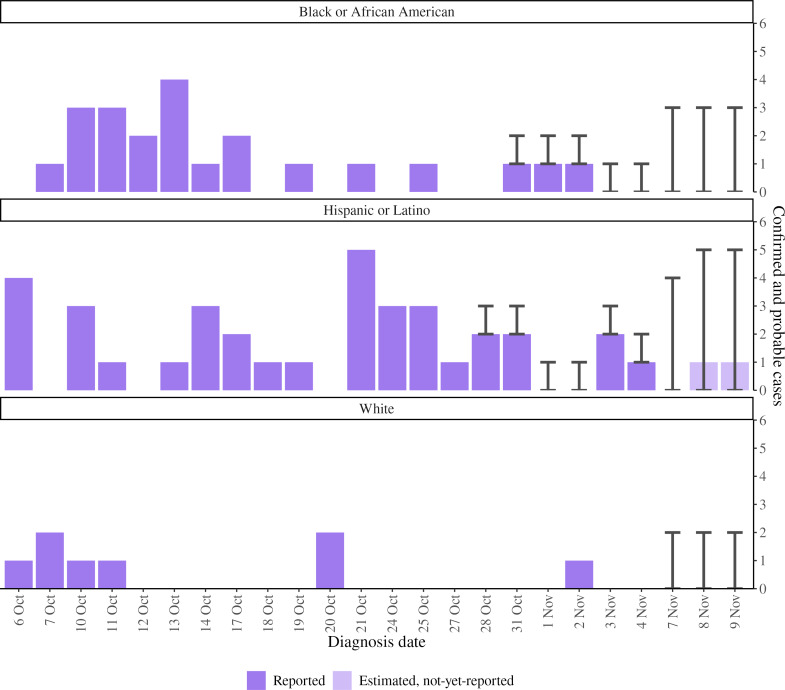
Background: Applying nowcasting methods to partially accrued reportable disease data can help policymakers interpret recent epidemic trends despite data lags and quickly identify and remediate health inequities. During the 2022 mpox outbreak in New York City, we applied Nowcasting by Bayesian Smoothing (NobBS) to estimate recent cases, citywide and stratified by race or ethnicity (Black or African American, Hispanic or Latino, and White). However, in real time, it was unclear if the estimates were accurate.
Objective: We evaluated the accuracy of estimated mpox case counts across a range of NobBS implementation options.
Methods: We evaluated NobBS performance for New York City residents with a confirmed or probable mpox diagnosis or illness onset from July 8 through September 30, 2022, as compared with fully accrued cases. We used the exponentiated average log score (average score) to compare moving window lengths, stratifying or not by race or ethnicity, diagnosis and onset dates, and daily and weekly aggregation.
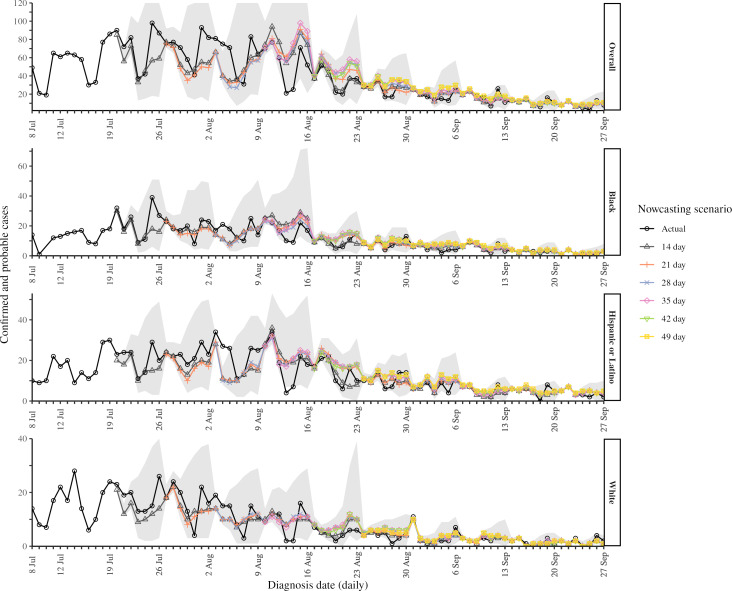
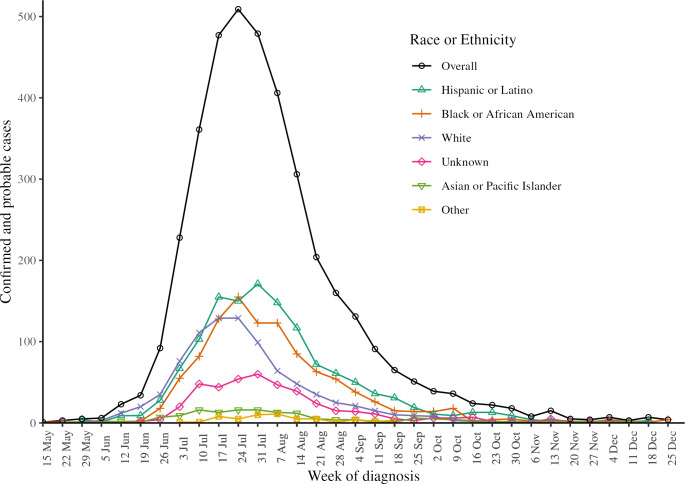
Results: During the study period, 3305 New York City residents were diagnosed with mpox (median 4, IQR 3-5 days from diagnosis to diagnosis report). Of these, 812 (25%) had missing onset dates, and of these, 230 (28%) had unknown race or ethnicity. The median lag in days from onset to onset report was 10 (IQR 7-14). For daily hindcasts by diagnosis date, the average score was 0.27 for the 14-day moving window used in real time. Average scores improved (increased) with longer moving windows (maximum: 0.47 for 49-day window). Stratifying by race or ethnicity improved performance, with an overall average score of 0.38 for the 14-day moving window (maximum: 0.57 for 49 day-window). Hindcasts for White patients performed best, with average scores of 0.45 for the 14-day window and 0.75 for the 49-day window. For unstratified, daily hindcasts by onset date, the average score ranged from 0.16 for the 42-day window to 0.30 for the 14-day window. Performance was not improved by weekly aggregation. Hindcasts underestimated diagnoses in early August after the epidemic peaked, then overestimated diagnoses in late August as the epidemic waned. Estimates were most accurate during September when cases were low and stable.
Conclusions: Performance was better when hindcasting by diagnosis date than by onset date, consistent with shorter lags and higher completeness for diagnoses. For daily hindcasts by diagnosis date, longer moving windows performed better, but direct comparisons are limited because longer windows could only be assessed after case counts in this outbreak had stabilized. Stratification by race or ethnicity improved performance and identified differences in epidemic trends across patient groups. Contributors to differences in performance across strata might include differences in case volume, epidemic trends, delay distributions, and interview success rates. Health departments need reliable nowcasting and rapid evaluation tools, particularly to promote health equity by ensuring accurate estimates within all strata.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


