Maria Phylactou, Luke Dixon, Catherine Rennie, Thang Han, Jyotsana Gaur, Niamh M Martin
{"title":"Ectopic Thyrotropin-Secreting Tumor in the Nasopharynx Causing Central Hyperthyroidism.","authors":"Maria Phylactou, Luke Dixon, Catherine Rennie, Thang Han, Jyotsana Gaur, Niamh M Martin","doi":"10.1210/jcemcr/luae250","DOIUrl":null,"url":null,"abstract":"<p><p>We report a 31-year-old man with diarrhea and tachycardia. Diagnostic workup confirmed raised free thyroid hormones with unsuppressed thyroid stimulating hormone (TSH). Laboratory assay and medication interference were excluded. Consistent with a high glycoprotein hormone α-subunit (α-GSU), the α-GSU:TSH molar ratio was increased. However, anterior pituitary panel testing also confirmed an isolated, raised follicle stimulating hormone (FSH) (17.3 IU/L; reference range, 1.7-8.0). Therefore, interpretation of α-GSU was limited given the co-existent elevated FSH. There was no pituitary lesion on magnetic resonance imaging (MRI) and stimulated TSH was 232% of baseline levels following thyrotropin-releasing hormone (TRH) stimulation, making a diagnosis of TSH-oma less likely. Genetic analysis revealed no pathogenic variants in the thyroid hormone receptor β gene. Due to the persistently elevated FSH, a follow-up pituitary MRI was arranged, which identified a nasopharyngeal mass on the floor of the sphenoid sinus, raising the possibility of ectopic pituitary tissue. The patient underwent endoscopic resection of this lesion, with subsequent normalization of free T4, TSH, and FSH within a few weeks. Histology confirmed a plurihormonal pituitary adenoma with staining for TSH, growth hormone, luteinizing hormone, and FSH. This case highlights the biochemical and radiological challenges of diagnosing ectopic TSH-secreting pituitary tumors.</p>","PeriodicalId":73540,"journal":{"name":"JCEM case reports","volume":"3 1","pages":"luae250"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11733770/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCEM case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1210/jcemcr/luae250","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
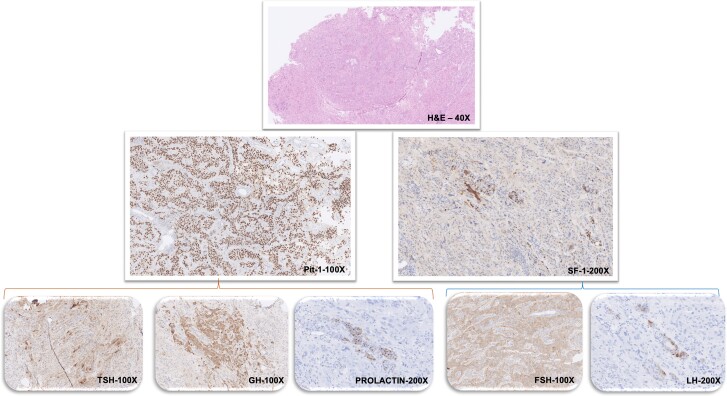
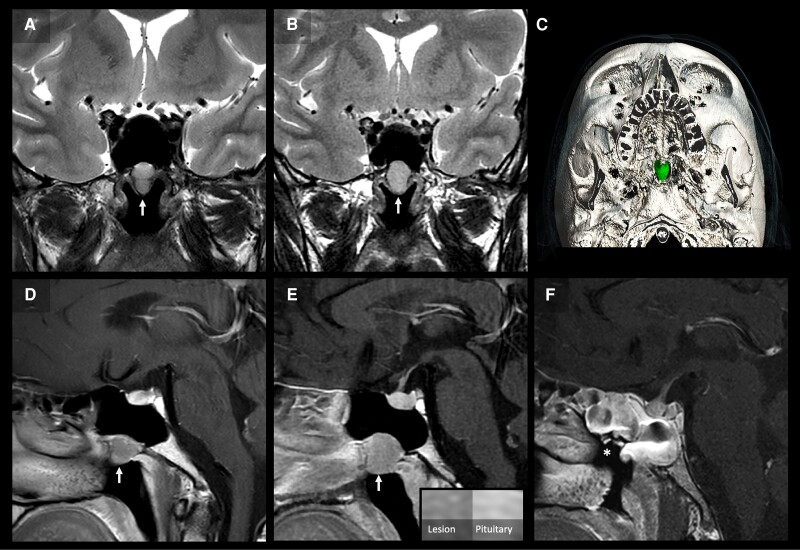
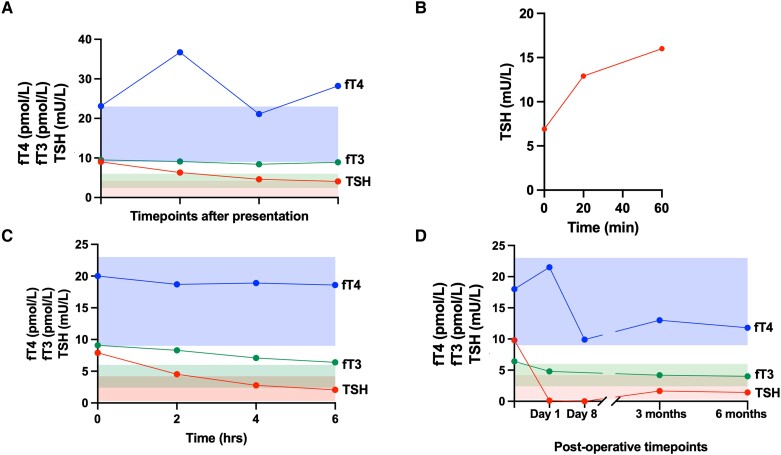
We report a 31-year-old man with diarrhea and tachycardia. Diagnostic workup confirmed raised free thyroid hormones with unsuppressed thyroid stimulating hormone (TSH). Laboratory assay and medication interference were excluded. Consistent with a high glycoprotein hormone α-subunit (α-GSU), the α-GSU:TSH molar ratio was increased. However, anterior pituitary panel testing also confirmed an isolated, raised follicle stimulating hormone (FSH) (17.3 IU/L; reference range, 1.7-8.0). Therefore, interpretation of α-GSU was limited given the co-existent elevated FSH. There was no pituitary lesion on magnetic resonance imaging (MRI) and stimulated TSH was 232% of baseline levels following thyrotropin-releasing hormone (TRH) stimulation, making a diagnosis of TSH-oma less likely. Genetic analysis revealed no pathogenic variants in the thyroid hormone receptor β gene. Due to the persistently elevated FSH, a follow-up pituitary MRI was arranged, which identified a nasopharyngeal mass on the floor of the sphenoid sinus, raising the possibility of ectopic pituitary tissue. The patient underwent endoscopic resection of this lesion, with subsequent normalization of free T4, TSH, and FSH within a few weeks. Histology confirmed a plurihormonal pituitary adenoma with staining for TSH, growth hormone, luteinizing hormone, and FSH. This case highlights the biochemical and radiological challenges of diagnosing ectopic TSH-secreting pituitary tumors.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


