Association of Time in Target Range of Resting Heart Rate With Adverse Clinical Outcomes in Patients With Acute Coronary Syndromes After Percutaneous Coronary Intervention.
{"title":"Association of Time in Target Range of Resting Heart Rate With Adverse Clinical Outcomes in Patients With Acute Coronary Syndromes After Percutaneous Coronary Intervention.","authors":"Jianmei Zheng, Cen Chen, Zhongcai Fan, Qiang Ye, Yi Zhong, Jinsong Li, Hao Huang, Jianping Deng, Jinghong Zhao, Tinglin Xiong, Wenjie Tian, Xuemei Zhang","doi":"10.5334/gh.1384","DOIUrl":null,"url":null,"abstract":"<p><p>Heart rate (HR) has been proved to be associated with major adverse cardiovascular events (MACE) in Acute coronary syndrome patients. However, the threshold value and clinical significance of time in target of resting heart rate (TTR-HR) remain insufficiently elucidated. Our study aimed to evaluate the independent association between TTR-HR and cardiovascular outcomes in the follow-up study of ACS. A total of 1455 ACS patients who underwent percutaneous coronary intervention (PCI) and were admitted to 22 hospitals between 2019 and 2022 were enrolled and followed up for 12 months. MACE was defined as a composite of cardiac death, nonfatal recurrent myocardial infarction, ischemic-driven revascularization, and ischemic stroke. The association between TTR-HR and cardiovascular outcomes was assessed using Cox regression model. Compared to patients with TTR-HR 0-50% and >50%-75%, patients with TTR-HR > 75%-100% were older and less alcohol user, less likely to use diuretics and anti-diabetic drugs, these patients had less comorbidities of hyperlipidemia, diabetes, heart failure, and cardiac shock. After 12 months follow up, the incidence of MACE and composite endpoint but not mortality was higher in patients with TTR-HR 0-50% and >50%-75% than those with TTR-HR > 75%-100%. After multivariate adjustment, TTR-HR [hazard ratio = 2.11, 95% CI: 1.19-3.74, p = 0.01] was independently associated with composite endpoint. In summary, our study demonstrates that TTR-HR holds significant prognostic value, with TTR-HR > 75%-100% being independently associated with reduced composite endpoint risk in ACS patients following PCI. These findings emphasize the importance of effective heart rate control in ACS patients following PCI.</p>","PeriodicalId":56018,"journal":{"name":"Global Heart","volume":"20 1","pages":"3"},"PeriodicalIF":3.1000,"publicationDate":"2025-01-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11740706/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Heart","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5334/gh.1384","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
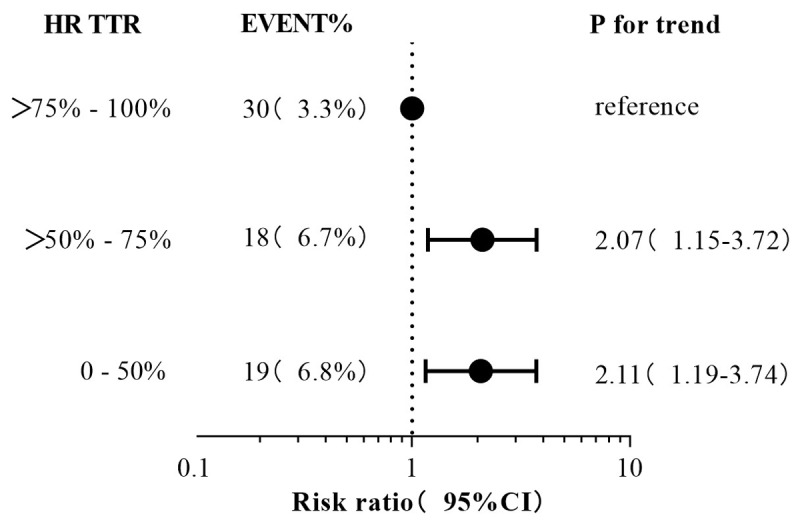
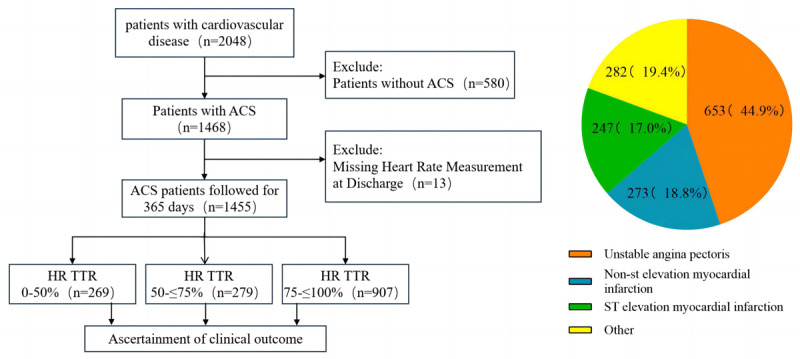
Heart rate (HR) has been proved to be associated with major adverse cardiovascular events (MACE) in Acute coronary syndrome patients. However, the threshold value and clinical significance of time in target of resting heart rate (TTR-HR) remain insufficiently elucidated. Our study aimed to evaluate the independent association between TTR-HR and cardiovascular outcomes in the follow-up study of ACS. A total of 1455 ACS patients who underwent percutaneous coronary intervention (PCI) and were admitted to 22 hospitals between 2019 and 2022 were enrolled and followed up for 12 months. MACE was defined as a composite of cardiac death, nonfatal recurrent myocardial infarction, ischemic-driven revascularization, and ischemic stroke. The association between TTR-HR and cardiovascular outcomes was assessed using Cox regression model. Compared to patients with TTR-HR 0-50% and >50%-75%, patients with TTR-HR > 75%-100% were older and less alcohol user, less likely to use diuretics and anti-diabetic drugs, these patients had less comorbidities of hyperlipidemia, diabetes, heart failure, and cardiac shock. After 12 months follow up, the incidence of MACE and composite endpoint but not mortality was higher in patients with TTR-HR 0-50% and >50%-75% than those with TTR-HR > 75%-100%. After multivariate adjustment, TTR-HR [hazard ratio = 2.11, 95% CI: 1.19-3.74, p = 0.01] was independently associated with composite endpoint. In summary, our study demonstrates that TTR-HR holds significant prognostic value, with TTR-HR > 75%-100% being independently associated with reduced composite endpoint risk in ACS patients following PCI. These findings emphasize the importance of effective heart rate control in ACS patients following PCI.
Global HeartMedicine-Cardiology and Cardiovascular Medicine
CiteScore
5.70
自引率
5.40%
发文量
77
审稿时长
5 weeks
期刊介绍:
Global Heart offers a forum for dialogue and education on research, developments, trends, solutions and public health programs related to the prevention and control of cardiovascular diseases (CVDs) worldwide, with a special focus on low- and middle-income countries (LMICs). Manuscripts should address not only the extent or epidemiology of the problem, but also describe interventions to effectively control and prevent CVDs and the underlying factors. The emphasis should be on approaches applicable in settings with limited resources.
Economic evaluations of successful interventions are particularly welcome. We will also consider negative findings if important. While reports of hospital or clinic-based treatments are not excluded, particularly if they have broad implications for cost-effective disease control or prevention, we give priority to papers addressing community-based activities. We encourage submissions on cardiovascular surveillance and health policies, professional education, ethical issues and technological innovations related to prevention.
Global Heart is particularly interested in publishing data from updated national or regional demographic health surveys, World Health Organization or Global Burden of Disease data, large clinical disease databases or registries. Systematic reviews or meta-analyses on globally relevant topics are welcome. We will also consider clinical research that has special relevance to LMICs, e.g. using validated instruments to assess health-related quality-of-life in patients from LMICs, innovative diagnostic-therapeutic applications, real-world effectiveness clinical trials, research methods (innovative methodologic papers, with emphasis on low-cost research methods or novel application of methods in low resource settings), and papers pertaining to cardiovascular health promotion and policy (quantitative evaluation of health programs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


