Oluwaseun Omoba, Ryan Farrell, William Chase Johnson, Samon Tavakoli, David Wallace, Viktor Bartanusz, Cristian Gragnaniello, Fassil B Mesfin, Michael McGinity
{"title":"Non-instrumented management of traumatic atlanto-axial rotatory subluxation: surgical technique.","authors":"Oluwaseun Omoba, Ryan Farrell, William Chase Johnson, Samon Tavakoli, David Wallace, Viktor Bartanusz, Cristian Gragnaniello, Fassil B Mesfin, Michael McGinity","doi":"10.21037/jss-24-44","DOIUrl":null,"url":null,"abstract":"<p><p>Atlantoaxial rotatory subluxation (AARS) in the adult population is primarily trauma-induced. Conservative and surgical treatments have both been used successfully in treating AARS. In cases where AARS cannot be reduced by conservative measures, open reduction and fusion is the conventional treatment approach. This report details a novel approach for treating adult AARS, where an open reduction was performed without instrumentation or fusion. The patient, a 48-year-old female involved in a high-speed vehicular collision, initially underwent conservative treatment with Gardner Wells Tongs and manual traction. Despite these efforts, X-ray and computed tomography (CT) scans indicated persistent subluxation. Subsequently, the patient was taken to the operating room, where successful open reduction was achieved without the need for fusion or instrumentation. Preoperative imaging revealed rotatory subluxation of C1-2 with a comminuted and displaced fracture of the right C1-2 facet joint and a nondisplaced fracture of the base of the occiput. The surgical technique involved precise manual manipulation using a Cloward spreader and real-time assessment with O-arm 3D X-ray tomography to ensure successful reduction. The absence of significant laxity or instability during intraoperative testing led to the conclusion that fusion was unnecessary. This approach minimizes invasive tissue dissection and preserves natural cervical range of motion (ROM). Postoperatively, the patient was asymptomatic with no joint instability and demonstrated satisfactory alignment at follow-up.</p>","PeriodicalId":17131,"journal":{"name":"Journal of spine surgery","volume":"10 4","pages":"697-705"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11732323/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of spine surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/jss-24-44","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/11 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
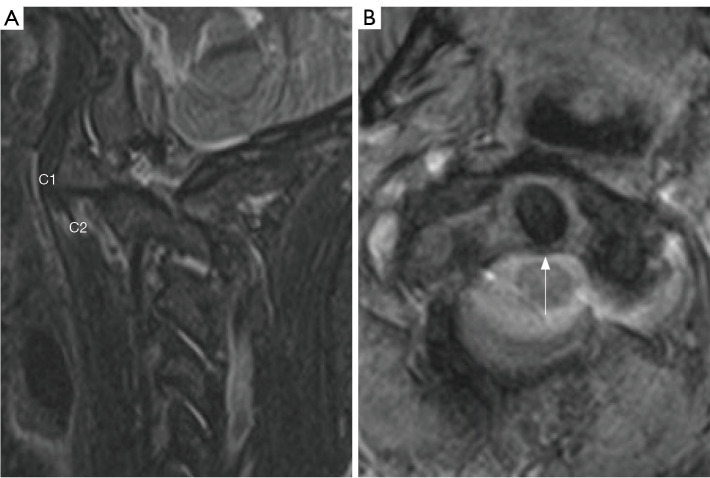
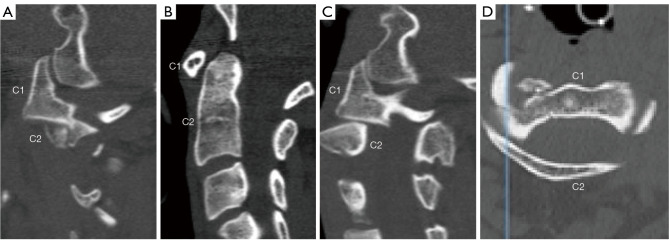
Atlantoaxial rotatory subluxation (AARS) in the adult population is primarily trauma-induced. Conservative and surgical treatments have both been used successfully in treating AARS. In cases where AARS cannot be reduced by conservative measures, open reduction and fusion is the conventional treatment approach. This report details a novel approach for treating adult AARS, where an open reduction was performed without instrumentation or fusion. The patient, a 48-year-old female involved in a high-speed vehicular collision, initially underwent conservative treatment with Gardner Wells Tongs and manual traction. Despite these efforts, X-ray and computed tomography (CT) scans indicated persistent subluxation. Subsequently, the patient was taken to the operating room, where successful open reduction was achieved without the need for fusion or instrumentation. Preoperative imaging revealed rotatory subluxation of C1-2 with a comminuted and displaced fracture of the right C1-2 facet joint and a nondisplaced fracture of the base of the occiput. The surgical technique involved precise manual manipulation using a Cloward spreader and real-time assessment with O-arm 3D X-ray tomography to ensure successful reduction. The absence of significant laxity or instability during intraoperative testing led to the conclusion that fusion was unnecessary. This approach minimizes invasive tissue dissection and preserves natural cervical range of motion (ROM). Postoperatively, the patient was asymptomatic with no joint instability and demonstrated satisfactory alignment at follow-up.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


