{"title":"Underuse of rapid sequence intubation outside emergency departments: preliminary, retrospective, observational study with emergency physician insights.","authors":"Sung-Yeol Park, Sung-Bin Chon","doi":"10.15441/ceem.24.227","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Rapid sequence intubation (RSI) involves the administration of induction agents and neuromuscular blockers before endotracheal intubation (ETI). However, RSI is underutilized outside emergency departments (EDs). We compared RSI adoption rates and ETI outcomes outside and within the EDs and investigated whether RSI adoption affected ETI outcomes outside the EDs.</p><p><strong>Methods: </strong>This retrospective study included adults who underwent emergency ETI outside the operating room at one university hospital between March 2022 and February 2023. The exclusion criteria included cardiopulmonary resuscitation, intentional RSI avoidance, and tube exchange via an introducer. The primary outcome was first-pass success rate. Secondary outcomes were multiple attempts (≥3), prolonged ETI (>5 minutes), and complications. The association between RSI adoption and outcomes outside the ED was assessed using multivariate logistic regression.</p><p><strong>Results: </strong>A total of 490 ETI cases was included: 286 occurred outside the ED and 204 within the ED. The mean age was 68.3±14.7 years and 290 were male. Cases outside the ED received fewer RSI attempts than cases within the ED (12.6% vs. 86.8%, P<0.001). The former showed fewer incidents of first-attempt success (62.2% vs. 88.2%, P<0.001), more numerous multiple attempts (11.5% vs. 2.0%, P<0.001), longer total time of ETI (8.4±8.3 minutes vs. 2.5±2.5 minutes, P<0.001), and more frequent complications (32.2% vs. 19.6%, P=0.003). However, multivariate logistic regression revealed no significant association between RSI adoption and these outcomes outside the ED: odds ratio, 1.74 (95% confidence interval [CI], 0.783-3.84), 0.167 (95% CI, 0.022-1.30), 1.04 (95% CI, 0.405-2.69), and 1.50 (95% CI, 0.664-3.40), respectively.</p><p><strong>Conclusion: </strong>Outside the ED, RSI adoption was lower and ETI outcomes were poorer than those within the ED. However, no association was found between RSI adoption and ETI outcomes outside the ED.</p>","PeriodicalId":10325,"journal":{"name":"Clinical and Experimental Emergency Medicine","volume":" ","pages":"139-147"},"PeriodicalIF":2.3000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12245651/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15441/ceem.24.227","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/14 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Rapid sequence intubation (RSI) involves the administration of induction agents and neuromuscular blockers before endotracheal intubation (ETI). However, RSI is underutilized outside emergency departments (EDs). We compared RSI adoption rates and ETI outcomes outside and within the EDs and investigated whether RSI adoption affected ETI outcomes outside the EDs.
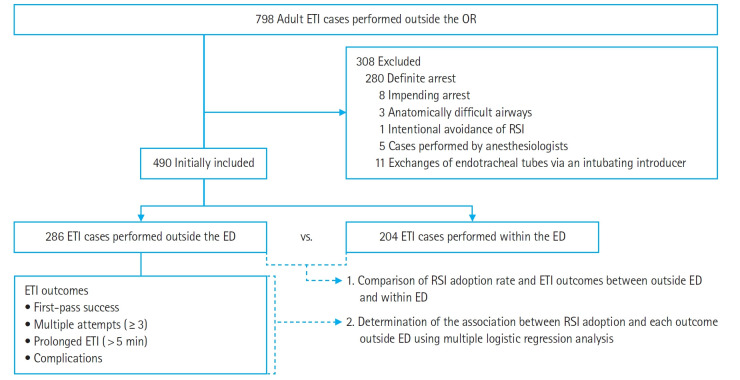
Methods: This retrospective study included adults who underwent emergency ETI outside the operating room at one university hospital between March 2022 and February 2023. The exclusion criteria included cardiopulmonary resuscitation, intentional RSI avoidance, and tube exchange via an introducer. The primary outcome was first-pass success rate. Secondary outcomes were multiple attempts (≥3), prolonged ETI (>5 minutes), and complications. The association between RSI adoption and outcomes outside the ED was assessed using multivariate logistic regression.
Results: A total of 490 ETI cases was included: 286 occurred outside the ED and 204 within the ED. The mean age was 68.3±14.7 years and 290 were male. Cases outside the ED received fewer RSI attempts than cases within the ED (12.6% vs. 86.8%, P<0.001). The former showed fewer incidents of first-attempt success (62.2% vs. 88.2%, P<0.001), more numerous multiple attempts (11.5% vs. 2.0%, P<0.001), longer total time of ETI (8.4±8.3 minutes vs. 2.5±2.5 minutes, P<0.001), and more frequent complications (32.2% vs. 19.6%, P=0.003). However, multivariate logistic regression revealed no significant association between RSI adoption and these outcomes outside the ED: odds ratio, 1.74 (95% confidence interval [CI], 0.783-3.84), 0.167 (95% CI, 0.022-1.30), 1.04 (95% CI, 0.405-2.69), and 1.50 (95% CI, 0.664-3.40), respectively.
Conclusion: Outside the ED, RSI adoption was lower and ETI outcomes were poorer than those within the ED. However, no association was found between RSI adoption and ETI outcomes outside the ED.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


