Alan Campbell, Diana Velazquez-Pimentel, Matthew Seager, Richard Hesketh, Julian Hague, Jowad Raja, Jocelyn Brookes, An Ngo, Miles Walkden, Anthie Papadopoulou, Daron Smith, Borzoueh Mohammadi, Ravi Barod, Mohammed Rashid Akhtar, Jimmy Kyaw Tun, Deborah Elise Low, Ian Daniel Renfrew, Tim Fotheringham, Conrad von Stempel
{"title":"Lymphatic leaks - success of intranodal lymphangiogram first strategy.","authors":"Alan Campbell, Diana Velazquez-Pimentel, Matthew Seager, Richard Hesketh, Julian Hague, Jowad Raja, Jocelyn Brookes, An Ngo, Miles Walkden, Anthie Papadopoulou, Daron Smith, Borzoueh Mohammadi, Ravi Barod, Mohammed Rashid Akhtar, Jimmy Kyaw Tun, Deborah Elise Low, Ian Daniel Renfrew, Tim Fotheringham, Conrad von Stempel","doi":"10.1186/s42155-024-00499-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Lymphatic leaks are associated with significant mortality and morbidity. Intranodal lymphangiography (ILAG) involves the direct injection of ethiodised lipid into the hilum of lymph nodes. It is diagnostic procedure that can have therapeutic effects secondary to a local sclerosant effect. The aim of the study is to describe the technical and clinical success of ILAG and adjunctive lymphatic interventions performed as first line interventional techniques for lymphatic leaks refractory to conservative and medical management in a multicentre cohort of patients with symptomatic large volume lymphatic leaks.</p><p><strong>Methods: </strong>Multicentre retrospective study of all lymphatic interventions performed between 2017-2023 in patients with large volume lymphatic leaks (> 500 ml a day). Intranodal lymphangiography was performed initially with technical success defined as opacification of the lymphatics at the aortic bifurcation and demonstration of lymphatic leak on the index ILAG procedure or immediate post procedural CT was recorded. Lymphatic embolisation was performed with a combination of direct puncture or transvenous cannulation with glue and or coil embolisation of the thoracic duct or leak point and in cases with refractory leak. Clinical success was defined as reduction in drain output to less than 20 mL per 24 h, or no further insensible lymph leak. Time to clinical success after ILAG and adjunctive embolisation was recorded.</p><p><strong>Results: </strong>ILAG alone lead to clinical success in 14 of 32 (44%) patients after a median of 14 days. Subsequent embolisation was performed in 12 refractory cases; this was successful in 8 (67%) at median of 8 days. Overall clinical success of all lymphatic interventions was 69% (22 of 32 patients) at a median of 11 days (IQR 5-34). No statistically significant correlation between the site of leakage, aetiology or embolisation technique correlated with clinical success. Decision to proceed to repeat ILAG or an adjunct procedure was made on a clinical basis, following multidisciplinary discussion.</p><p><strong>Conclusions: </strong>ILAG can be employed a first line interventional therapeutic technique to treat clinically significant lymphatic leaks that are refractory to conservative and medical management. Adjunctive procedures, including embolisation, can be considered as part of clinical decision making after a period of 1-2 weeks' watchful waiting in continuingly refractory cases.</p>","PeriodicalId":52351,"journal":{"name":"CVIR Endovascular","volume":"8 1","pages":"4"},"PeriodicalIF":1.5000,"publicationDate":"2025-01-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11718034/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CVIR Endovascular","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42155-024-00499-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
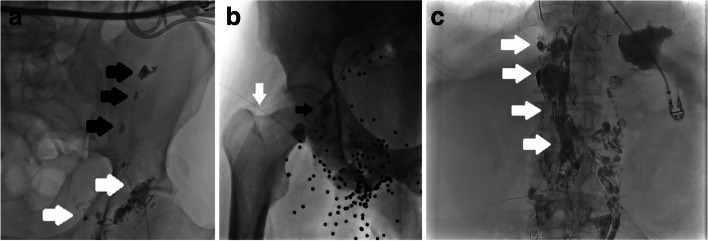
Background: Lymphatic leaks are associated with significant mortality and morbidity. Intranodal lymphangiography (ILAG) involves the direct injection of ethiodised lipid into the hilum of lymph nodes. It is diagnostic procedure that can have therapeutic effects secondary to a local sclerosant effect. The aim of the study is to describe the technical and clinical success of ILAG and adjunctive lymphatic interventions performed as first line interventional techniques for lymphatic leaks refractory to conservative and medical management in a multicentre cohort of patients with symptomatic large volume lymphatic leaks.
Methods: Multicentre retrospective study of all lymphatic interventions performed between 2017-2023 in patients with large volume lymphatic leaks (> 500 ml a day). Intranodal lymphangiography was performed initially with technical success defined as opacification of the lymphatics at the aortic bifurcation and demonstration of lymphatic leak on the index ILAG procedure or immediate post procedural CT was recorded. Lymphatic embolisation was performed with a combination of direct puncture or transvenous cannulation with glue and or coil embolisation of the thoracic duct or leak point and in cases with refractory leak. Clinical success was defined as reduction in drain output to less than 20 mL per 24 h, or no further insensible lymph leak. Time to clinical success after ILAG and adjunctive embolisation was recorded.
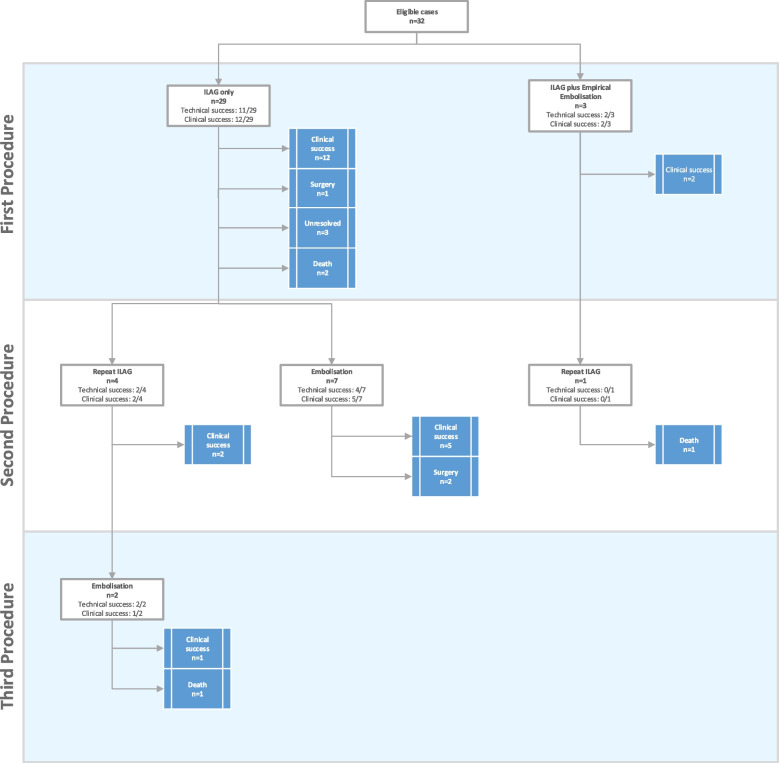
Results: ILAG alone lead to clinical success in 14 of 32 (44%) patients after a median of 14 days. Subsequent embolisation was performed in 12 refractory cases; this was successful in 8 (67%) at median of 8 days. Overall clinical success of all lymphatic interventions was 69% (22 of 32 patients) at a median of 11 days (IQR 5-34). No statistically significant correlation between the site of leakage, aetiology or embolisation technique correlated with clinical success. Decision to proceed to repeat ILAG or an adjunct procedure was made on a clinical basis, following multidisciplinary discussion.
Conclusions: ILAG can be employed a first line interventional therapeutic technique to treat clinically significant lymphatic leaks that are refractory to conservative and medical management. Adjunctive procedures, including embolisation, can be considered as part of clinical decision making after a period of 1-2 weeks' watchful waiting in continuingly refractory cases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


