Fatima M Damagum, Zainab D Ahmed, Rabiu I Jalo, Hamisu M Salihu, C William Wester, Muktar H Aliyu
{"title":"Adapted Counseling Care Model for Management of Female Sexual Dysfunction Among Women Living With and Without HIV.","authors":"Fatima M Damagum, Zainab D Ahmed, Rabiu I Jalo, Hamisu M Salihu, C William Wester, Muktar H Aliyu","doi":"10.25259/IJMA_37_2024","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objective: </strong>Sexual health research among women living with human immunodeficiency virus (HIV) has focused mainly on sexual practices and risk behaviors, with little consideration for treating sexual dysfunction and improving sexual satisfaction. The aim of this pilot study was to assess the effectiveness of an adaptive counseling care model in the management of female sexual dysfunction (FSD) among women living with HIV and without HIV in northern Nigeria.</p><p><strong>Methods: </strong>This was a prospective cohort study of 200 women with HIV and a matched comparison arm of 200 women without HIV. Sexual function was assessed using the Female Sexual Function Index (FSFI), with a score ≤ 26.55 indicating FSD. We counseled women with FSD using the Permission, Limited Information, Specific Suggestions, Intensive Therapy (PLISSIT) model and evaluated the effectiveness of the model by comparing mean differences in baseline and six weeks post-intervention FSFI scores.</p><p><strong>Results: </strong>The overall prevalence of FSD was 96.8%, with no difference between HIV-positive and HIV-negative participants (<i>p</i> = 0.398). Based on the six domains of the FSFI, the most common reported dysfunctions were sexual pain (21.7%), sexual desire disorder (17.6%), orgasm disorder (17.6%), lubrication disorder (17.2%), sexual arousal (16.9%), and poor sexual satisfaction (9.0%). The overall mean FSFI score (±standard deviation, SD) for those with FSD, in both groups (<i>n</i> = 387) prior to the counseling intervention was 16.05±10.65 (HIV-positive: 18.58±8.46; HIV-negative: 13.98±10.85). At the end of the intervention, the overall mean FSFI score in both groups increased to 23.58±16.53 (HIV-positive: 21.37±11.24; HIV-negative: 16.72±13.81) (<i>p</i> < 0.05 in all cases).</p><p><strong>Conclusion and global health implications: </strong>FSD is very common among women in Northern Nigeria, irrespective of HIV status. An adapted counseling care model improved sexual function in both HIV-positive and HIV-negative women. The PLISSIT model can guide healthcare providers to initiate and navigate sexual health discussions with women in this setting.</p>","PeriodicalId":30480,"journal":{"name":"International Journal of MCH and AIDS","volume":"13 ","pages":"e025"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11705164/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of MCH and AIDS","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.25259/IJMA_37_2024","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objective: Sexual health research among women living with human immunodeficiency virus (HIV) has focused mainly on sexual practices and risk behaviors, with little consideration for treating sexual dysfunction and improving sexual satisfaction. The aim of this pilot study was to assess the effectiveness of an adaptive counseling care model in the management of female sexual dysfunction (FSD) among women living with HIV and without HIV in northern Nigeria.
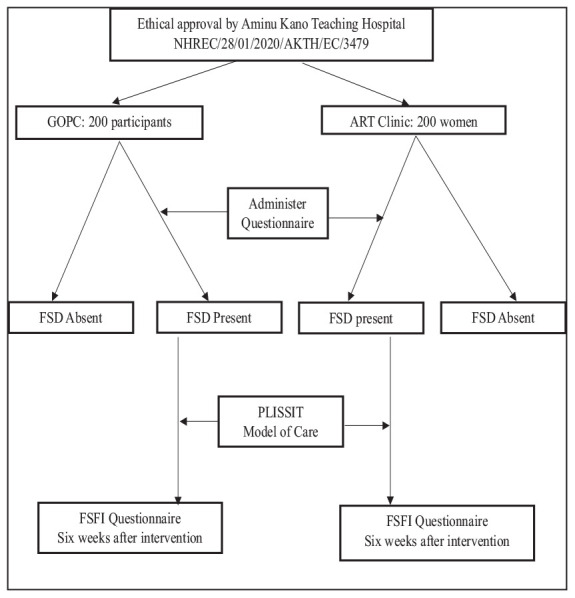
Methods: This was a prospective cohort study of 200 women with HIV and a matched comparison arm of 200 women without HIV. Sexual function was assessed using the Female Sexual Function Index (FSFI), with a score ≤ 26.55 indicating FSD. We counseled women with FSD using the Permission, Limited Information, Specific Suggestions, Intensive Therapy (PLISSIT) model and evaluated the effectiveness of the model by comparing mean differences in baseline and six weeks post-intervention FSFI scores.
Results: The overall prevalence of FSD was 96.8%, with no difference between HIV-positive and HIV-negative participants (p = 0.398). Based on the six domains of the FSFI, the most common reported dysfunctions were sexual pain (21.7%), sexual desire disorder (17.6%), orgasm disorder (17.6%), lubrication disorder (17.2%), sexual arousal (16.9%), and poor sexual satisfaction (9.0%). The overall mean FSFI score (±standard deviation, SD) for those with FSD, in both groups (n = 387) prior to the counseling intervention was 16.05±10.65 (HIV-positive: 18.58±8.46; HIV-negative: 13.98±10.85). At the end of the intervention, the overall mean FSFI score in both groups increased to 23.58±16.53 (HIV-positive: 21.37±11.24; HIV-negative: 16.72±13.81) (p < 0.05 in all cases).
Conclusion and global health implications: FSD is very common among women in Northern Nigeria, irrespective of HIV status. An adapted counseling care model improved sexual function in both HIV-positive and HIV-negative women. The PLISSIT model can guide healthcare providers to initiate and navigate sexual health discussions with women in this setting.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


