{"title":"Simple methods for estimating the maximum 24-hour urinary potassium excretion in kidney failure without replacement therapy patients.","authors":"Danyang Zhang, Yukun Wang, Shimin Jiang, Wenge Li","doi":"10.1080/0886022X.2024.2445157","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Adjusting dietary potassium intake based on 24-hour urinary potassium excretion is the primary method of preventing hyperkalemia. Currently, there is no accurate and convenient method for calculating maximum 24-hour urinary potassium excretion in kidney failure without replacement therapy patients. We developed and validated two new models to assess the upper limit of dietary potassium consumption in this high-risk cohort, using the maximum 24-hour urinary potassium excretion as a proxy.</p><p><strong>Methods: </strong>The data of 145 kidney failure without replacement therapy patients with hyperkalemia was gathered. The prediction models were developed using multilayer perceptron and stepwise multiple linear regression utilizing a stochastic sample of 102 (70%) patients. Within the rest 43 (30%), the performance of various models was independently verified.</p><p><strong>Results: </strong>The two new models had low bias (-0.02 and -0.57 mmol/24h vs 66.74 and 79.91 mmol/24h, mean absolute error = 5.57 and 5.22 vs 68.95 and 81.37), high accuracy (percentage of calculated values within_±30% of measured values = 83.45% and 84.14% vs 0.00% and 0.00%), high correlation with measured values (Spearman correlation coefficient = 0.72 and 0.72 vs 0.46 and 0.45, intraclass correlation coefficient = 0.67 and 0.70 vs 0.03 and 0.03) and high agreement with 24-hour urine potassium measurements (95% limits of agreement of Bland-Altman plot = 13.70 and 13.20 mmol/24h vs 113.8 and 191.3 mmol/24h).</p><p><strong>Conclusion: </strong>These new models show high clinical application value for the calculation of maximum 24-hour urinary potassium excretion in kidney failure without replacement therapy patients with hyperkalemia.</p>","PeriodicalId":20839,"journal":{"name":"Renal Failure","volume":"47 1","pages":"2445157"},"PeriodicalIF":3.0000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11721948/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Renal Failure","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1080/0886022X.2024.2445157","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/8 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Adjusting dietary potassium intake based on 24-hour urinary potassium excretion is the primary method of preventing hyperkalemia. Currently, there is no accurate and convenient method for calculating maximum 24-hour urinary potassium excretion in kidney failure without replacement therapy patients. We developed and validated two new models to assess the upper limit of dietary potassium consumption in this high-risk cohort, using the maximum 24-hour urinary potassium excretion as a proxy.
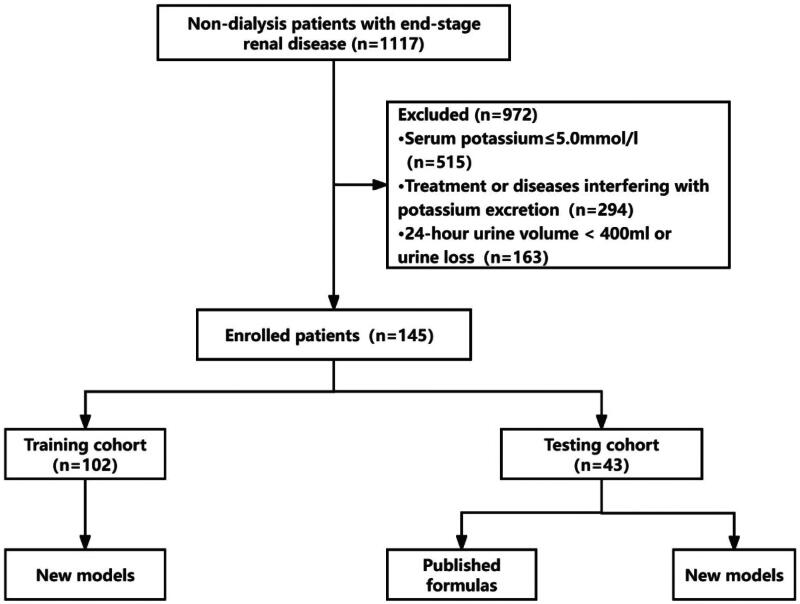
Methods: The data of 145 kidney failure without replacement therapy patients with hyperkalemia was gathered. The prediction models were developed using multilayer perceptron and stepwise multiple linear regression utilizing a stochastic sample of 102 (70%) patients. Within the rest 43 (30%), the performance of various models was independently verified.
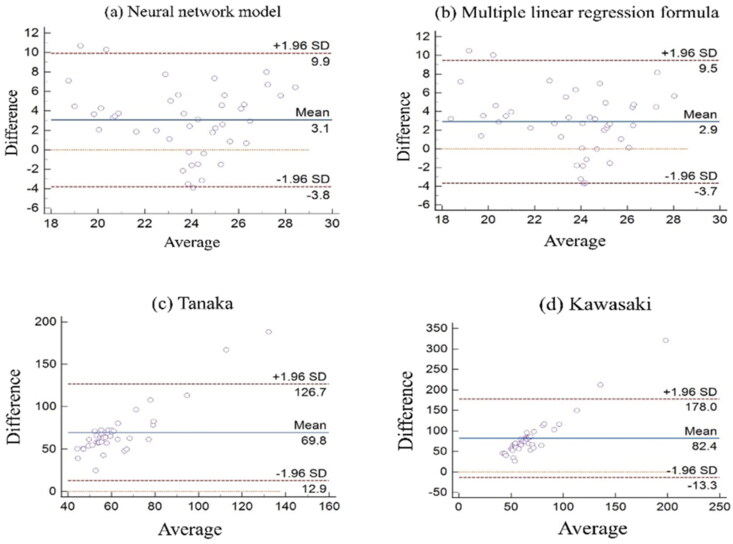
Results: The two new models had low bias (-0.02 and -0.57 mmol/24h vs 66.74 and 79.91 mmol/24h, mean absolute error = 5.57 and 5.22 vs 68.95 and 81.37), high accuracy (percentage of calculated values within_±30% of measured values = 83.45% and 84.14% vs 0.00% and 0.00%), high correlation with measured values (Spearman correlation coefficient = 0.72 and 0.72 vs 0.46 and 0.45, intraclass correlation coefficient = 0.67 and 0.70 vs 0.03 and 0.03) and high agreement with 24-hour urine potassium measurements (95% limits of agreement of Bland-Altman plot = 13.70 and 13.20 mmol/24h vs 113.8 and 191.3 mmol/24h).
Conclusion: These new models show high clinical application value for the calculation of maximum 24-hour urinary potassium excretion in kidney failure without replacement therapy patients with hyperkalemia.
背景:根据24小时尿钾排泄量调整膳食钾摄入量是预防高钾血症的主要方法。目前,没有准确方便的方法来计算未经替代治疗的肾衰竭患者24小时最大尿钾排泄量。我们开发并验证了两种新的模型,以24小时最大尿钾排泄量为指标,评估高危人群饮食钾摄入量的上限。方法:收集145例未经替代治疗的肾衰合并高钾血症患者的资料。利用102例(70%)患者的随机样本,采用多层感知器和逐步多元线性回归建立预测模型。在其余43个(30%)中,各模型的性能被独立验证。结果:两种新模型偏差低(分别为-0.02和-0.57 mmol/24h vs 66.74和79.91 mmol/24h,平均绝对误差分别为5.57和5.22 vs 68.95和81.37),准确度高(计算值与实测值在±30%范围内的百分比分别为83.45%和84.14% vs 0.00%和0.00%),与实测值相关性高(Spearman相关系数分别为0.72和0.72 vs 0.46和0.45)。类内相关系数分别为0.67和0.70 (vs 0.03和0.03),且与24小时尿钾测量值高度吻合(Bland-Altman图95%一致性限分别为13.70和13.20 mmol/24h vs 113.8和191.3 mmol/24h)。结论:这些新模型对未接受替代治疗的肾功能衰竭伴高钾血症患者24小时最大尿钾排泄量的计算具有较高的临床应用价值。
期刊介绍:
Renal Failure primarily concentrates on acute renal injury and its consequence, but also addresses advances in the fields of chronic renal failure, hypertension, and renal transplantation. Bringing together both clinical and experimental aspects of renal failure, this publication presents timely, practical information on pathology and pathophysiology of acute renal failure; nephrotoxicity of drugs and other substances; prevention, treatment, and therapy of renal failure; renal failure in association with transplantation, hypertension, and diabetes mellitus.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


