Vikram K Raghu, Scott D Rothenberger, James E Squires, Elizabeth Eisenberg, Anna L Peters, Jennifer Halma, Swati Antala, Irini D Batsis, Ke-You Zhang, Amy G Feldman, Daniel H Leung, Steven J Lobritto, John Bucuvalas, Simon P Horslen, George V Mazariegos, Emily R Perito
{"title":"Association Between Early Immunosuppression Center Variability and One-Year Outcomes After Pediatric Liver Transplant.","authors":"Vikram K Raghu, Scott D Rothenberger, James E Squires, Elizabeth Eisenberg, Anna L Peters, Jennifer Halma, Swati Antala, Irini D Batsis, Ke-You Zhang, Amy G Feldman, Daniel H Leung, Steven J Lobritto, John Bucuvalas, Simon P Horslen, George V Mazariegos, Emily R Perito","doi":"10.1111/petr.70018","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Despite the existence of institutional protocols, liver transplant centers often have variability in early immunosuppression practices. We aimed to measure within-center variability in early immunosuppression after pediatric liver transplant (LT) and examine its association with one-year outcomes.</p><p><strong>Methods: </strong>We analyzed pediatric LTs from 2013 to 2018 in the United Network for Organ Sharing registry, with data aggregated by center. We categorized induction regimen as corticosteroids only vs. T-cell depleting antibody vs. non-T-cell depleting antibody. Primary exposures were coefficient of immunosuppression variability (CIV) in (1) induction and (2) mycophenolate mofetil (MMF) use. Primary outcomes were one-year graft survival, patient survival, and acute rejection rate within the first year after transplant.</p><p><strong>Results: </strong>The study cohort included 2542 LT recipients from 67 LT centers. Sixteen centers (24%) had no MMF variability; twenty-five centers (37%) had no induction variability. In multivariable analysis, induction CIV was associated with 2.72 times greater odds of acute rejection in the first year (OR 2.72; 95% CI 1.66-4.45; p < 0.001). MMF CIV was not associated with rejection (OR 1.22, 95% CI 0.66-2.25, p = 0.527). Neither one-year graft nor patient survival were associated with induction or MMF CIV.</p><p><strong>Conclusions: </strong>Induction CIV is associated with higher one-year acute rejection odds and did not impact short-term graft or patient survival. Improved understanding of the reasons for high CIV will inform future work aiming to determine whether reducing variability may improve outcomes.</p>","PeriodicalId":20038,"journal":{"name":"Pediatric Transplantation","volume":"29 1","pages":"e70018"},"PeriodicalIF":1.4000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11707728/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Transplantation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/petr.70018","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Despite the existence of institutional protocols, liver transplant centers often have variability in early immunosuppression practices. We aimed to measure within-center variability in early immunosuppression after pediatric liver transplant (LT) and examine its association with one-year outcomes.
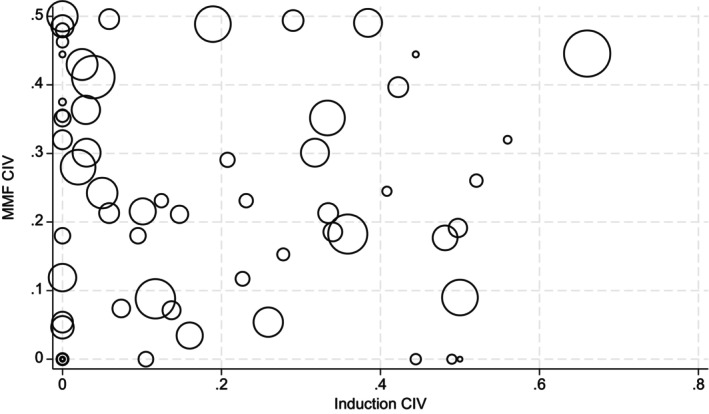
Methods: We analyzed pediatric LTs from 2013 to 2018 in the United Network for Organ Sharing registry, with data aggregated by center. We categorized induction regimen as corticosteroids only vs. T-cell depleting antibody vs. non-T-cell depleting antibody. Primary exposures were coefficient of immunosuppression variability (CIV) in (1) induction and (2) mycophenolate mofetil (MMF) use. Primary outcomes were one-year graft survival, patient survival, and acute rejection rate within the first year after transplant.
Results: The study cohort included 2542 LT recipients from 67 LT centers. Sixteen centers (24%) had no MMF variability; twenty-five centers (37%) had no induction variability. In multivariable analysis, induction CIV was associated with 2.72 times greater odds of acute rejection in the first year (OR 2.72; 95% CI 1.66-4.45; p < 0.001). MMF CIV was not associated with rejection (OR 1.22, 95% CI 0.66-2.25, p = 0.527). Neither one-year graft nor patient survival were associated with induction or MMF CIV.
Conclusions: Induction CIV is associated with higher one-year acute rejection odds and did not impact short-term graft or patient survival. Improved understanding of the reasons for high CIV will inform future work aiming to determine whether reducing variability may improve outcomes.
背景:尽管存在机构协议,肝移植中心在早期免疫抑制实践中往往存在差异。我们旨在测量儿童肝移植(LT)后早期免疫抑制的中心内变异性,并检查其与一年预后的关系。方法:我们分析了2013年至2018年在美国器官共享网络登记的儿童LTs,并按中心汇总数据。我们将诱导方案分为仅皮质类固醇、t细胞消耗抗体和非t细胞消耗抗体。在(1)诱导和(2)使用霉酚酸酯(MMF)时,主要暴露于免疫抑制变异性系数(CIV)。主要结局是1年的移植物存活率、患者存活率和移植后1年内的急性排异率。结果:研究队列包括来自67个肝移植中心的2542名肝移植受者。16个中心(24%)没有MMF变异性;25个中心(37%)没有诱导变异性。在多变量分析中,诱导CIV与第一年急性排斥反应的几率增加2.72倍相关(OR 2.72;95% ci 1.66-4.45;结论:诱导CIV与较高的1年急性排斥发生率相关,且不影响短期移植或患者生存。提高对高CIV原因的理解将为未来的工作提供信息,旨在确定减少变异是否可以改善结果。
期刊介绍:
The aim of Pediatric Transplantation is to publish original articles of the highest quality on clinical experience and basic research in transplantation of tissues and solid organs in infants, children and adolescents. The journal seeks to disseminate the latest information widely to all individuals involved in kidney, liver, heart, lung, intestine and stem cell (bone-marrow) transplantation. In addition, the journal publishes focused reviews on topics relevant to pediatric transplantation as well as timely editorial comment on controversial issues.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


