{"title":"The Impact on Patient Prognosis of Changes to the Method of Notifying Staff About Accepting Patients With Out-of-Hospital Cardiac Arrest.","authors":"Youichi Inoue, Keisuke Okamura, Hideaki Shimada, Shinobu Watakabe, Shiori Hirayama, Machiko Hirata, Ayaka Kusuda, Arisa Matsumoto, Miki Inoue, Emi Matsuishi, Mizuki Yamada, Sachiko Iwanaga, Shogo Narumi, Shiki Nakayama, Hideto Sako, Akihiro Udo, Kenichiro Taniguchi, Shogo Morisaki, Souichiro Ide, Yasuyuki Nomoto, Shin-Ichiro Miura, Osamu Imakyure, Ichiro Imamura","doi":"10.14740/jocmr6111","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Our hospital is a designated emergency hospital and accepts many patients with out-of-hospital cardiac arrest (OHCA). Previously, after receiving a direct call from emergency services to request acceptance of an OHCA patient, the emergency room (ER) chief nurse notified medical staff. However, this method delayed ER preparations, so a Code Blue system (CB) was introduced in which the pending arrival of an OHCA patient was broadcast throughout the hospital.</p><p><strong>Methods: </strong>In this study, we retrospectively analyzed the impact of introducing CB at our hospital on OHCA patient prognosis to examine whether the introduction of CB is clinically meaningful. We compared consecutive cases treated before introduction of the CB (March 3, 2022, to March 22, 2023) with those treated afterwards (March 23, 2023, to July 23, 2024).</p><p><strong>Results: </strong>A total of 30 cases per group were included. The mean number of medical staff present at admissions increased significantly from 5.4 ± 0.6 to 15.0 ± 3.0 (P < 0.001). Although not statistically significant, the introduction of the CB increased the return of spontaneous circulation (ROSC) rate from 20% to 30%, survival to discharge rate from 3% to 10%, and social reintegration rate from 0% to 3%. ROSC occurred in 15 patients. Among OHCA patients with cardiac disease, the ROSC rate tended to increase from 0% to 43% (P = 0.055). In addition, in OHCA patients with cardiac disease whose electrocardiogram initially showed ventricular fibrillation or pulseless electrical activity, the ROSC rate increased from 0% to 100%. ROSC tended to be influenced by the total number of staff and physicians present and the number of staff such as medical clerks, clinical engineers, and radiology technicians (P = 0.095, 0.076, 0.088, respectively).</p><p><strong>Conclusions: </strong>Introduction of a CB may increase the ROSC rate and the number of patients surviving to discharge. It also appears to improve the quality of medical care by quickly gathering all necessary medical staff so that they can perform their predefined roles.</p>","PeriodicalId":94329,"journal":{"name":"Journal of clinical medicine research","volume":"16 12","pages":"578-588"},"PeriodicalIF":2.0000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11699870/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of clinical medicine research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jocmr6111","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/20 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
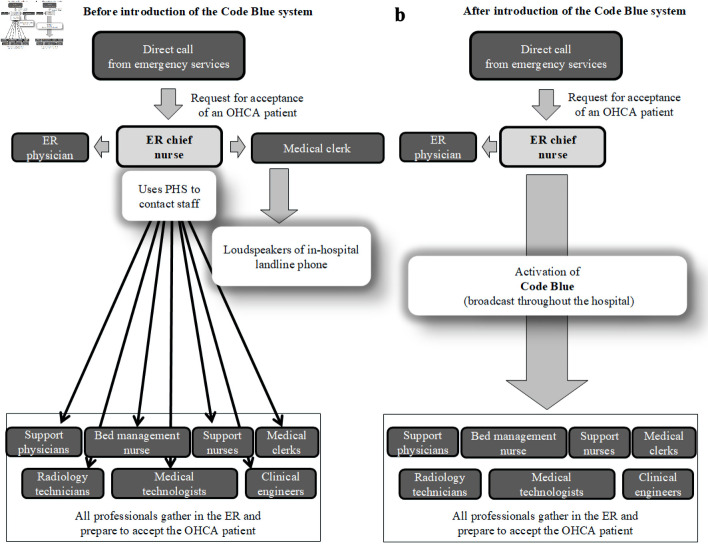
Background: Our hospital is a designated emergency hospital and accepts many patients with out-of-hospital cardiac arrest (OHCA). Previously, after receiving a direct call from emergency services to request acceptance of an OHCA patient, the emergency room (ER) chief nurse notified medical staff. However, this method delayed ER preparations, so a Code Blue system (CB) was introduced in which the pending arrival of an OHCA patient was broadcast throughout the hospital.
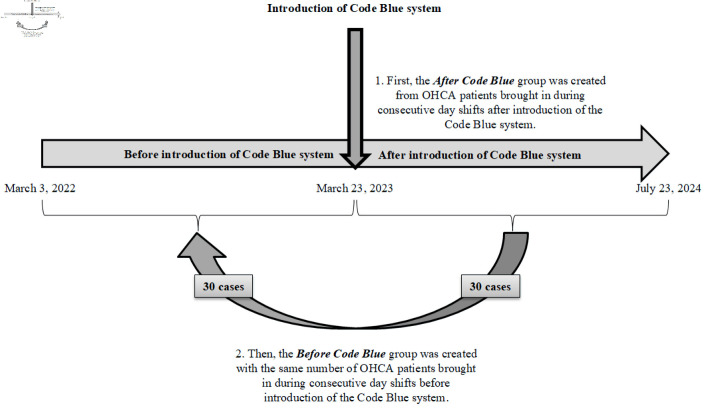
Methods: In this study, we retrospectively analyzed the impact of introducing CB at our hospital on OHCA patient prognosis to examine whether the introduction of CB is clinically meaningful. We compared consecutive cases treated before introduction of the CB (March 3, 2022, to March 22, 2023) with those treated afterwards (March 23, 2023, to July 23, 2024).
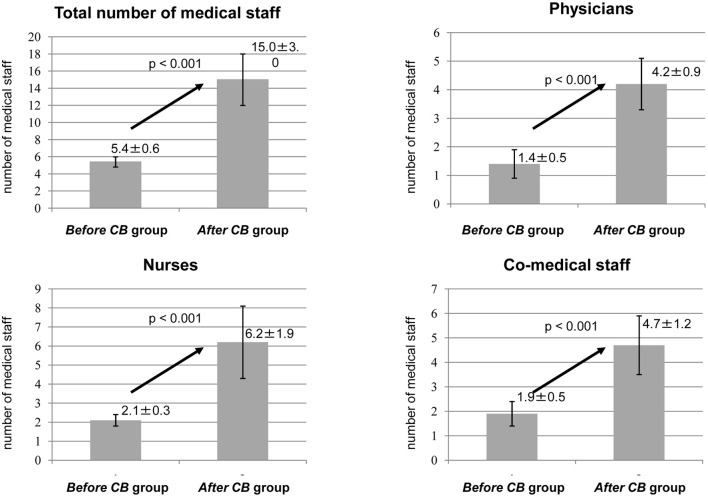
Results: A total of 30 cases per group were included. The mean number of medical staff present at admissions increased significantly from 5.4 ± 0.6 to 15.0 ± 3.0 (P < 0.001). Although not statistically significant, the introduction of the CB increased the return of spontaneous circulation (ROSC) rate from 20% to 30%, survival to discharge rate from 3% to 10%, and social reintegration rate from 0% to 3%. ROSC occurred in 15 patients. Among OHCA patients with cardiac disease, the ROSC rate tended to increase from 0% to 43% (P = 0.055). In addition, in OHCA patients with cardiac disease whose electrocardiogram initially showed ventricular fibrillation or pulseless electrical activity, the ROSC rate increased from 0% to 100%. ROSC tended to be influenced by the total number of staff and physicians present and the number of staff such as medical clerks, clinical engineers, and radiology technicians (P = 0.095, 0.076, 0.088, respectively).
Conclusions: Introduction of a CB may increase the ROSC rate and the number of patients surviving to discharge. It also appears to improve the quality of medical care by quickly gathering all necessary medical staff so that they can perform their predefined roles.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


