Association Between Chronic Kidney Disease Risk Categories and Abdominal Aortic Calcification: Insights From the National Health and Nutrition Examination Survey.
Song Peng Ang, Jackson Rajendran, Jia Ee Chia, Pratiksha Singh, Jose Iglesias
{"title":"Association Between Chronic Kidney Disease Risk Categories and Abdominal Aortic Calcification: Insights From the National Health and Nutrition Examination Survey.","authors":"Song Peng Ang, Jackson Rajendran, Jia Ee Chia, Pratiksha Singh, Jose Iglesias","doi":"10.14740/jocmr6101","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Abdominal aortic calcification (AAC) is a critical indicator of cardiovascular risk, particularly in patients with chronic kidney disease (CKD). Traditional classification systems may underestimate the risk in those with moderate CKD. This study aimed to evaluate the association between CKD risk categories - defined by both estimated glomerular filtration rate (eGFR) and albuminuria - and the prevalence of severe AAC.</p><p><strong>Methods: </strong>This cross-sectional study analyzed data from the National Health and Nutrition Examination Survey (NHANES) 2013-2014. We included adults aged ≥ 40 years who underwent imaging for AAC assessment, excluding pregnant individuals and those without AAC scores. Survey-weighted and multivariate logistic regression was employed to assess the relationship between CKD risk categories and severe AAC, adjusting for age, hypertension, and smoking history. Subgroup analyses were conducted to explore variability across demographic and clinical subgroups.</p><p><strong>Results: </strong>We analyzed data from 3,140 participants in the NHANES, 423 (13.4%) of whom had severe AAC. The cohort was categorized into CKD risk categories 1 through 4, with the majority (76%) in stage 1. Severe AAC was more prevalent among older individuals and those with traditional cardiovascular risk factors. Initial unadjusted analyses revealed that CKD category 2 was associated with a nearly fourfold increase in severe AAC (odds ratio (OR): 3.93), while categories 3 and 4 showed 3.75-fold and over 10-fold increases, respectively (all P < 0.01). However, after adjusting for confounders, categories 2 and 4 showed higher risks of severe AAC compared to category 1, but these associations did not reach statistical significance (OR: 1.72, 95% confidence interval (CI): 0.90 - 1.86, P = 0.06 and OR: 5.70, 95% CI: 0.85 - 38.00, P = 0.07, respectively).</p><p><strong>Conclusion: </strong>Our study offers insights that may complement the current reliance on eGFR and albuminuria in risk stratification, highlighting that CKD category 2, defined by mildly reduced eGFR and albuminuria, may be a potential marker for severe AAC. Although statistical significance was narrowly missed after full adjustment, the clinical implications remain significant, advocating for more aggressive cardiovascular risk management in this population. This understanding may contribute to evolving approaches in CKD-related cardiovascular risk assessment and inform potential intervention strategies.</p>","PeriodicalId":94329,"journal":{"name":"Journal of clinical medicine research","volume":"16 12","pages":"589-599"},"PeriodicalIF":2.0000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11699866/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of clinical medicine research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jocmr6101","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/20 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Abdominal aortic calcification (AAC) is a critical indicator of cardiovascular risk, particularly in patients with chronic kidney disease (CKD). Traditional classification systems may underestimate the risk in those with moderate CKD. This study aimed to evaluate the association between CKD risk categories - defined by both estimated glomerular filtration rate (eGFR) and albuminuria - and the prevalence of severe AAC.
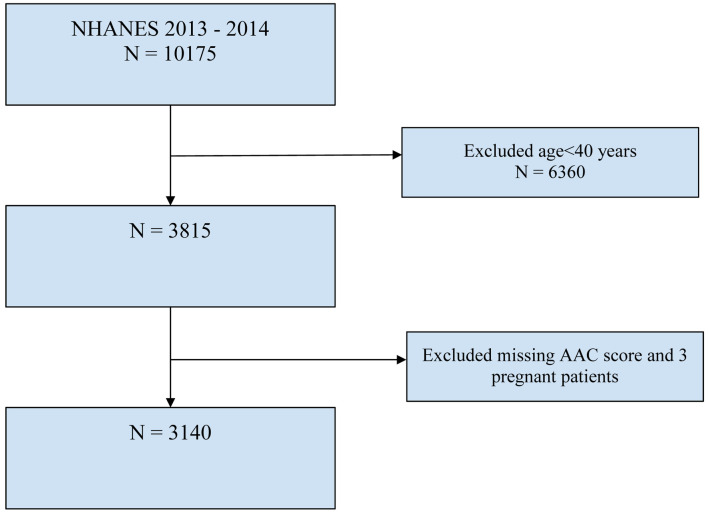
Methods: This cross-sectional study analyzed data from the National Health and Nutrition Examination Survey (NHANES) 2013-2014. We included adults aged ≥ 40 years who underwent imaging for AAC assessment, excluding pregnant individuals and those without AAC scores. Survey-weighted and multivariate logistic regression was employed to assess the relationship between CKD risk categories and severe AAC, adjusting for age, hypertension, and smoking history. Subgroup analyses were conducted to explore variability across demographic and clinical subgroups.
Results: We analyzed data from 3,140 participants in the NHANES, 423 (13.4%) of whom had severe AAC. The cohort was categorized into CKD risk categories 1 through 4, with the majority (76%) in stage 1. Severe AAC was more prevalent among older individuals and those with traditional cardiovascular risk factors. Initial unadjusted analyses revealed that CKD category 2 was associated with a nearly fourfold increase in severe AAC (odds ratio (OR): 3.93), while categories 3 and 4 showed 3.75-fold and over 10-fold increases, respectively (all P < 0.01). However, after adjusting for confounders, categories 2 and 4 showed higher risks of severe AAC compared to category 1, but these associations did not reach statistical significance (OR: 1.72, 95% confidence interval (CI): 0.90 - 1.86, P = 0.06 and OR: 5.70, 95% CI: 0.85 - 38.00, P = 0.07, respectively).
Conclusion: Our study offers insights that may complement the current reliance on eGFR and albuminuria in risk stratification, highlighting that CKD category 2, defined by mildly reduced eGFR and albuminuria, may be a potential marker for severe AAC. Although statistical significance was narrowly missed after full adjustment, the clinical implications remain significant, advocating for more aggressive cardiovascular risk management in this population. This understanding may contribute to evolving approaches in CKD-related cardiovascular risk assessment and inform potential intervention strategies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


