Pre-Transplant Immune Dysregulation Predicts for Poor Outcome Following Allogeneic Haematopoietic Stem Cell Transplantation in Adolescents and Adults with Inborn Errors of Immunity (IEI).
Thomas A Fox, Valerie Massey, Charley Lever, Rachel Pearce, Arian Laurence, Sarah Grace, Filippo Oliviero, Sarita Workman, Andrew Symes, David M Lowe, Valeria Fiaccadori, Rachael Hough, Susan Tadros, Siobhan O Burns, Markus G Seidel, Ben Carpenter, Emma C Morris
{"title":"Pre-Transplant Immune Dysregulation Predicts for Poor Outcome Following Allogeneic Haematopoietic Stem Cell Transplantation in Adolescents and Adults with Inborn Errors of Immunity (IEI).","authors":"Thomas A Fox, Valerie Massey, Charley Lever, Rachel Pearce, Arian Laurence, Sarah Grace, Filippo Oliviero, Sarita Workman, Andrew Symes, David M Lowe, Valeria Fiaccadori, Rachael Hough, Susan Tadros, Siobhan O Burns, Markus G Seidel, Ben Carpenter, Emma C Morris","doi":"10.1007/s10875-024-01854-y","DOIUrl":null,"url":null,"abstract":"<p><p>Allogeneic haematopoietic stem cell transplantation (alloHSCT) is safe and effective for adolescents and adults with inborn errors of immunity (IEI) with severe disease manifestations of their disease. The haematopoietic cell transplantation comorbidity index (HCT-CI) score predicts transplant survival in non-malignant diseases, including IEIs. We hypothesised that immune dysregulation pre-transplant may also influence transplant outcomes. We calculated the pre-transplant immune dysregulation and disease activity score (IDDA v2.1) for 82 adolescent and adult IEI patients (aged ≥ 13 years). Three-year overall survival (OS) for the whole cohort was 90% (n = 82) with a median follow up of 44.7 months (range 8.4 to 225.8). Events were defined as acute graft-versus-host disease (GvHD) grades II or above, chronic GvHD of any grade, graft failure, or death from any cause. Three-year event free survival (EFS) for the whole cohort was 72%. In multivariable analysis the IDDA v2.1 score pre-transplant and HCT-CI score significantly impacted OS (hazard ratio 1.08, p = 0.028) and EFS (hazard ratio 1.04, p = 0.0005). Importantly, 35% of this cohort had a high IDDA v2.1 score (≥ 15) and low HCT-CI score (< 3) suggesting that the risks of alloHSCT may be underestimated in a proportion of patients with IEI if the HCT-CI score is used alone. These findings support the potential for improved outcomes following successful modulation of immune dysregulation pre-transplant. The IDDA v2.1 score has utility as an objective measurement of pre-transplant immune dysregulation providing additional information reagrding the risks and potential complications of alloHSCT in an individual IEI patient.</p>","PeriodicalId":15531,"journal":{"name":"Journal of Clinical Immunology","volume":"45 1","pages":"64"},"PeriodicalIF":5.7000,"publicationDate":"2025-01-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11703937/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Immunology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10875-024-01854-y","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
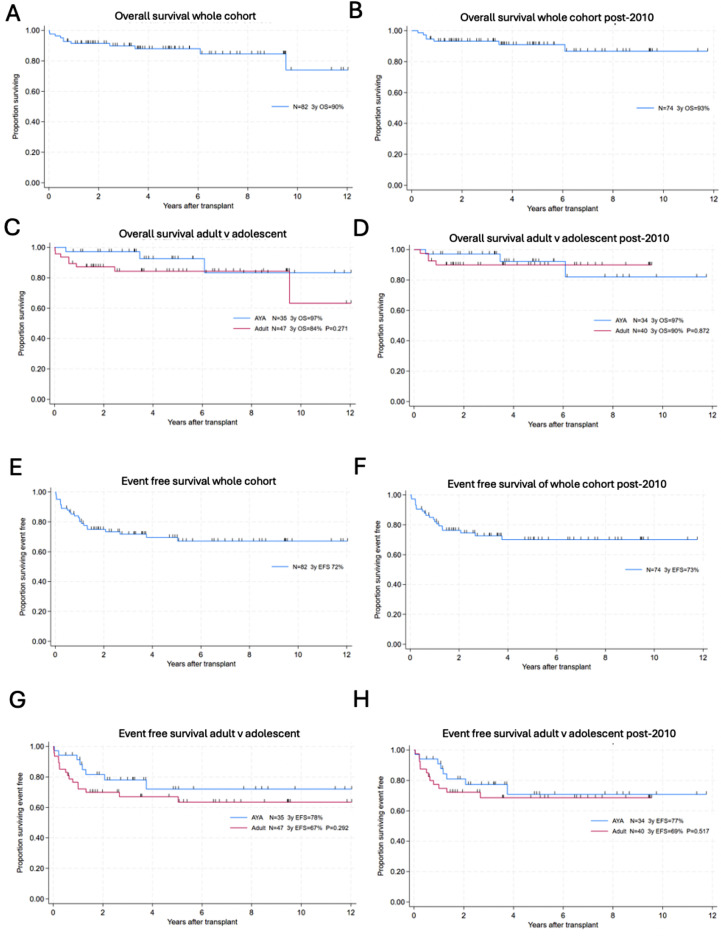
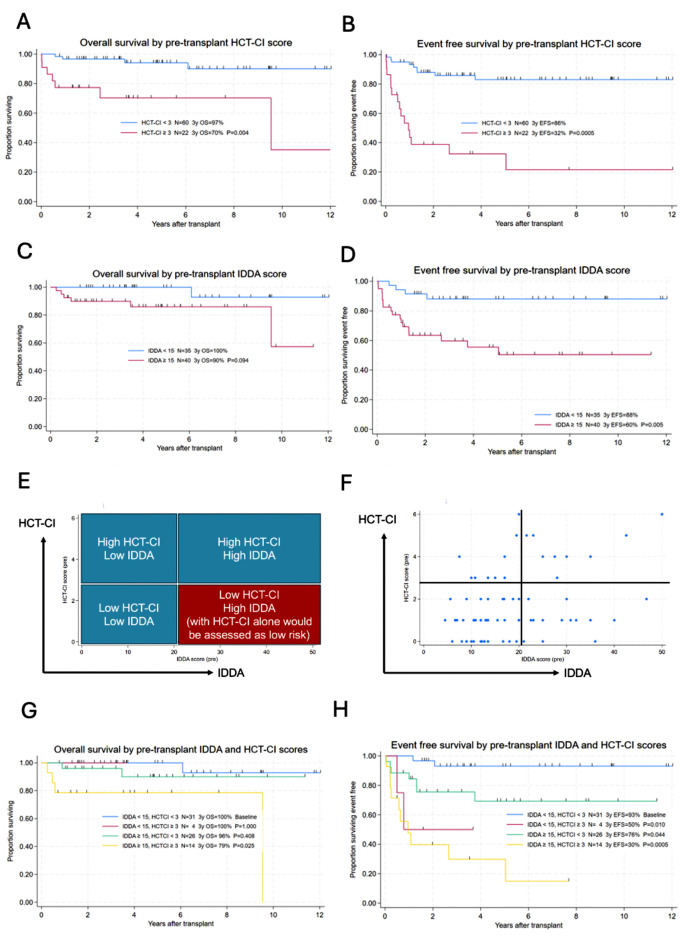
Allogeneic haematopoietic stem cell transplantation (alloHSCT) is safe and effective for adolescents and adults with inborn errors of immunity (IEI) with severe disease manifestations of their disease. The haematopoietic cell transplantation comorbidity index (HCT-CI) score predicts transplant survival in non-malignant diseases, including IEIs. We hypothesised that immune dysregulation pre-transplant may also influence transplant outcomes. We calculated the pre-transplant immune dysregulation and disease activity score (IDDA v2.1) for 82 adolescent and adult IEI patients (aged ≥ 13 years). Three-year overall survival (OS) for the whole cohort was 90% (n = 82) with a median follow up of 44.7 months (range 8.4 to 225.8). Events were defined as acute graft-versus-host disease (GvHD) grades II or above, chronic GvHD of any grade, graft failure, or death from any cause. Three-year event free survival (EFS) for the whole cohort was 72%. In multivariable analysis the IDDA v2.1 score pre-transplant and HCT-CI score significantly impacted OS (hazard ratio 1.08, p = 0.028) and EFS (hazard ratio 1.04, p = 0.0005). Importantly, 35% of this cohort had a high IDDA v2.1 score (≥ 15) and low HCT-CI score (< 3) suggesting that the risks of alloHSCT may be underestimated in a proportion of patients with IEI if the HCT-CI score is used alone. These findings support the potential for improved outcomes following successful modulation of immune dysregulation pre-transplant. The IDDA v2.1 score has utility as an objective measurement of pre-transplant immune dysregulation providing additional information reagrding the risks and potential complications of alloHSCT in an individual IEI patient.
期刊介绍:
The Journal of Clinical Immunology publishes impactful papers in the realm of human immunology, delving into the diagnosis, pathogenesis, prognosis, or treatment of human diseases. The journal places particular emphasis on primary immunodeficiencies and related diseases, encompassing inborn errors of immunity in a broad sense, their underlying genotypes, and diverse phenotypes. These phenotypes include infection, malignancy, allergy, auto-inflammation, and autoimmunity. We welcome a broad spectrum of studies in this domain, spanning genetic discovery, clinical description, immunologic assessment, diagnostic approaches, prognosis evaluation, and treatment interventions. Case reports are considered if they are genuinely original and accompanied by a concise review of the relevant medical literature, illustrating how the novel case study advances the field. The instructions to authors provide detailed guidance on the four categories of papers accepted by the journal.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


