The Hemodynamic Management and Postoperative Outcomes After Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy: A Prospective Observational Study.
Sohan Lal Solanki, Vandana Agarwal, Reshma P Ambulkar, Malini P Joshi, Shreyas Chawathey, Shivacharan Patel Rudrappa, Manish Bhandare, Avanish P Saklani
{"title":"The Hemodynamic Management and Postoperative Outcomes After Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy: A Prospective Observational Study.","authors":"Sohan Lal Solanki, Vandana Agarwal, Reshma P Ambulkar, Malini P Joshi, Shreyas Chawathey, Shivacharan Patel Rudrappa, Manish Bhandare, Avanish P Saklani","doi":"10.1155/ccrp/8815211","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (CRS-HIPEC) has become standard treatment for peritoneal cancers and metastases, significantly enhancing survival rates. This study evaluated the relationship between tumor burden, hemodynamic management, and postoperative outcomes after CRS-HIPEC. <b>Methodology:</b> This study included 203 patients undergoing CRS-HIPEC. The study was registered with ClinicalTrials.gov (NCT02754115). Routine and advanced hemodynamic monitoring was performed. Data on fluid and blood transfusions, coagulation management, body temperature, blood gases, Peritoneal Carcinomatosis Index (PCI), and chemotherapeutic agents used were collected. Postoperatively, complications using the Clavien-Dindo classification were employed. Primary outcomes assessed PCI's impact on hemodynamic parameters and fluid management, with secondary outcomes including postoperative complications, mortality, and length of ICU and hospital stays. <b>Results:</b> Patients with PCI > 20 experienced significantly longer surgeries (796.2 ± 158.3 min) as compared with patients with PCI 0-10 (551 ± 127 min) and patients with PCI between 11 and 20 (661.78 ± 137.7 min) (<i>p</i> ≤ 0.01). Patients with PCI > 20 received higher fluid requirements (mean: 5497.7 ± 2401.9 mL) as compared with PCI 0-10 (2631.2 ± 1459.9 mL) and PCI 10-20 (3964.65 ± 2044.6 mL) (<i>p</i> ≤ 0.01). Patients with PCI > 20 also had a prolonged ICU stays (median: 4 days) as compared with PCI 0-20 (median: 3 days). However, these differences were not significant in patients with PCI between 10 and 20. Significant differences in CI and SVI were observed among PCI groups during and after HIPEC. Significant differences were also observed among PCI groups for postoperative complications. Although 30-day survival rates varied clinically, they did not reach statistical significance. <b>Conclusion:</b> A higher PCI score was significantly associated with increased duration of surgery, fluid requirements, the need for invasive hemodynamic monitoring, postoperative complications, and longer ICU stays. Tailoring perioperative strategies based on PCI scores has the potential to optimize these outcomes. <b>Trial Registration:</b> ClinicalTrials.gov identifier: NCT02754115.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":"2024 ","pages":"8815211"},"PeriodicalIF":1.8000,"publicationDate":"2024-12-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11698608/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/ccrp/8815211","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
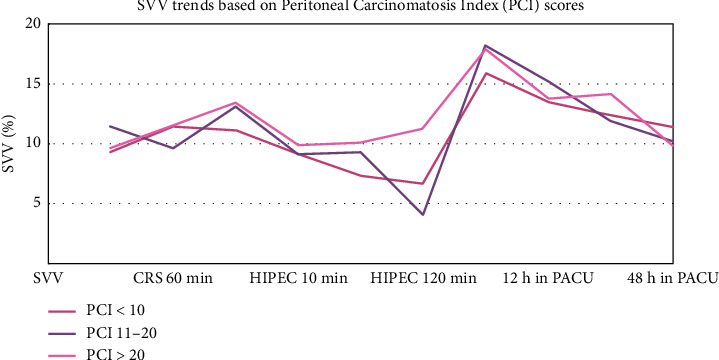
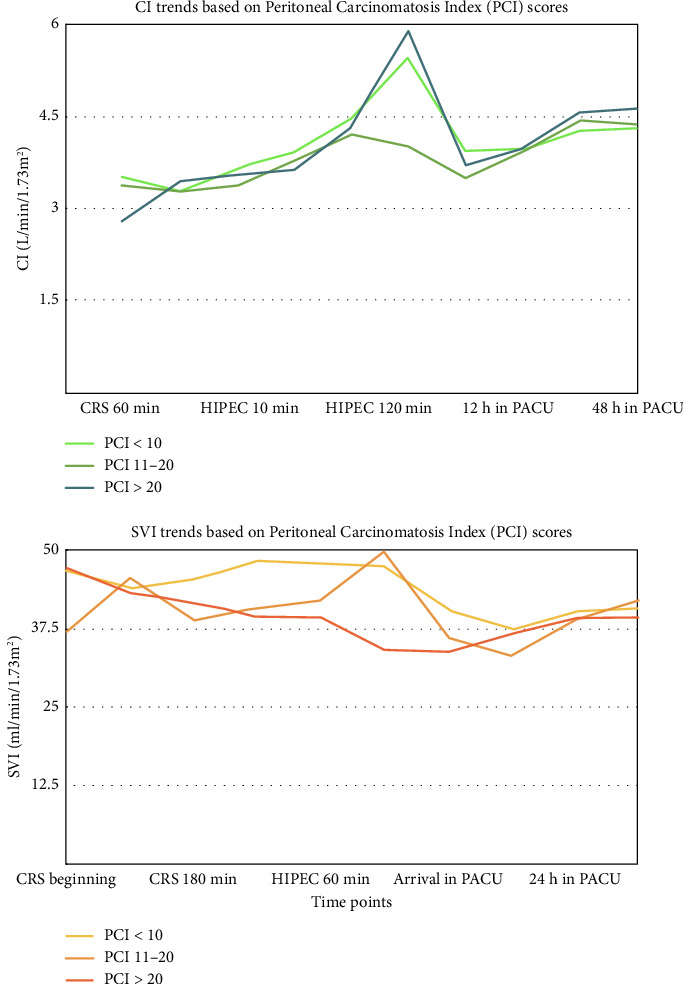
Background: Cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (CRS-HIPEC) has become standard treatment for peritoneal cancers and metastases, significantly enhancing survival rates. This study evaluated the relationship between tumor burden, hemodynamic management, and postoperative outcomes after CRS-HIPEC. Methodology: This study included 203 patients undergoing CRS-HIPEC. The study was registered with ClinicalTrials.gov (NCT02754115). Routine and advanced hemodynamic monitoring was performed. Data on fluid and blood transfusions, coagulation management, body temperature, blood gases, Peritoneal Carcinomatosis Index (PCI), and chemotherapeutic agents used were collected. Postoperatively, complications using the Clavien-Dindo classification were employed. Primary outcomes assessed PCI's impact on hemodynamic parameters and fluid management, with secondary outcomes including postoperative complications, mortality, and length of ICU and hospital stays. Results: Patients with PCI > 20 experienced significantly longer surgeries (796.2 ± 158.3 min) as compared with patients with PCI 0-10 (551 ± 127 min) and patients with PCI between 11 and 20 (661.78 ± 137.7 min) (p ≤ 0.01). Patients with PCI > 20 received higher fluid requirements (mean: 5497.7 ± 2401.9 mL) as compared with PCI 0-10 (2631.2 ± 1459.9 mL) and PCI 10-20 (3964.65 ± 2044.6 mL) (p ≤ 0.01). Patients with PCI > 20 also had a prolonged ICU stays (median: 4 days) as compared with PCI 0-20 (median: 3 days). However, these differences were not significant in patients with PCI between 10 and 20. Significant differences in CI and SVI were observed among PCI groups during and after HIPEC. Significant differences were also observed among PCI groups for postoperative complications. Although 30-day survival rates varied clinically, they did not reach statistical significance. Conclusion: A higher PCI score was significantly associated with increased duration of surgery, fluid requirements, the need for invasive hemodynamic monitoring, postoperative complications, and longer ICU stays. Tailoring perioperative strategies based on PCI scores has the potential to optimize these outcomes. Trial Registration: ClinicalTrials.gov identifier: NCT02754115.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


