Brief Report: Resolution of Neuropsychiatric Adverse Events After Switching to a Doravirine-Based Regimen in the Open-Label Extensions of the DRIVE-AHEAD and DRIVE-FORWARD Trials.
Graeme Moyle, Fanxia Meng, Hong Wan, Peter Sklar, Rebeca M Plank, Rima Lahoulou
{"title":"Brief Report: Resolution of Neuropsychiatric Adverse Events After Switching to a Doravirine-Based Regimen in the Open-Label Extensions of the DRIVE-AHEAD and DRIVE-FORWARD Trials.","authors":"Graeme Moyle, Fanxia Meng, Hong Wan, Peter Sklar, Rebeca M Plank, Rima Lahoulou","doi":"10.1097/QAI.0000000000003599","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Neuropsychiatric adverse events (NPAEs) are associated with several antiretrovirals. Doravirine (DOR), a non-nucleoside reverse transcriptase inhibitor indicated for HIV-1 treatment, does not interact significantly with known neurotransmitter receptors in vitro. First-line therapy with DOR-based regimens resulted in significantly fewer NPAEs than efavirenz/emtricitabine/tenofovir disoproxil fumarate (EFV/FTC/TDF) and similar rates to those of ritonavir-boosted darunavir (DRV/r) with 2 nucleos(t)ide reverse transcriptase inhibitors (NRTIs) through week 96 of the phase 3 DRIVE-AHEAD and DRIVE-FORWARD studies, respectively.</p><p><strong>Methods: </strong>In the DRIVE-AHEAD (NCT02403674) and DRIVE-FORWARD studies (NCT02275780), treatment-naive adults randomly received DOR/lamivudine/TDF or EFV/FTC/TDF and DOR + 2 NRTIs or DRV/r + 2 NRTIs, respectively, for a 96-week double-blind phase; afterward, participants could continue or switch to a DOR-based regimen for a 96-week open-label extension.</p><p><strong>Results: </strong>Overall, 269 and 233 participants in the DRIVE-AHEAD and DRIVE-FORWARD studies, respectively, switched to a DOR-based regimen. At week 96, 26 and 15 participants randomized to EFV/FTC/TDF and DRV/r + 2 NRTIs, respectively, had ongoing NPAEs, resolving by week 192 in 73% (19/26) and 40% (6/15) of participants switching to a DOR-based regimen. New-onset NPAEs were reported by 9% (25/269) and 8% (18/233) of participants; by week 192, new-onset NPAEs were resolved and/or resolving in 60% (15/25) and 61% (11/18) of participants.</p><p><strong>Conclusions: </strong>In both trial extensions, NPAEs persisted in 3%-4% of participants 96 weeks after switching to a DOR-based regimen, possibly representing the background rate for these events. This suggests that DOR-based therapy may be a good option for adults with baseline neuropsychiatric symptoms or those experiencing NPAEs with other antiretrovirals.</p>","PeriodicalId":14588,"journal":{"name":"JAIDS Journal of Acquired Immune Deficiency Syndromes","volume":" ","pages":"81-86"},"PeriodicalIF":2.2000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11970612/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAIDS Journal of Acquired Immune Deficiency Syndromes","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/QAI.0000000000003599","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Neuropsychiatric adverse events (NPAEs) are associated with several antiretrovirals. Doravirine (DOR), a non-nucleoside reverse transcriptase inhibitor indicated for HIV-1 treatment, does not interact significantly with known neurotransmitter receptors in vitro. First-line therapy with DOR-based regimens resulted in significantly fewer NPAEs than efavirenz/emtricitabine/tenofovir disoproxil fumarate (EFV/FTC/TDF) and similar rates to those of ritonavir-boosted darunavir (DRV/r) with 2 nucleos(t)ide reverse transcriptase inhibitors (NRTIs) through week 96 of the phase 3 DRIVE-AHEAD and DRIVE-FORWARD studies, respectively.
Methods: In the DRIVE-AHEAD (NCT02403674) and DRIVE-FORWARD studies (NCT02275780), treatment-naive adults randomly received DOR/lamivudine/TDF or EFV/FTC/TDF and DOR + 2 NRTIs or DRV/r + 2 NRTIs, respectively, for a 96-week double-blind phase; afterward, participants could continue or switch to a DOR-based regimen for a 96-week open-label extension.
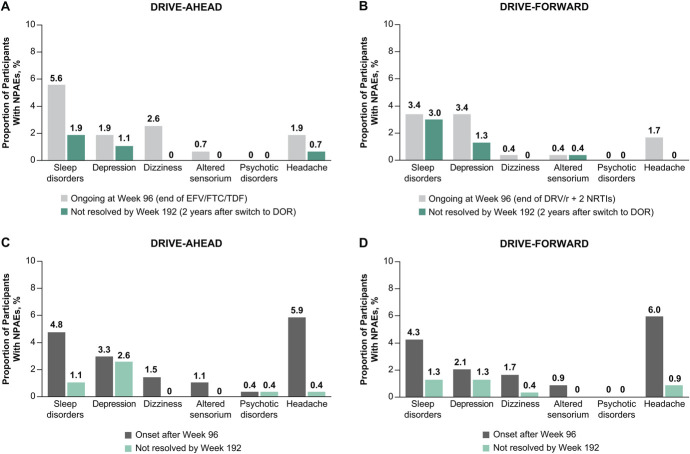
Results: Overall, 269 and 233 participants in the DRIVE-AHEAD and DRIVE-FORWARD studies, respectively, switched to a DOR-based regimen. At week 96, 26 and 15 participants randomized to EFV/FTC/TDF and DRV/r + 2 NRTIs, respectively, had ongoing NPAEs, resolving by week 192 in 73% (19/26) and 40% (6/15) of participants switching to a DOR-based regimen. New-onset NPAEs were reported by 9% (25/269) and 8% (18/233) of participants; by week 192, new-onset NPAEs were resolved and/or resolving in 60% (15/25) and 61% (11/18) of participants.
Conclusions: In both trial extensions, NPAEs persisted in 3%-4% of participants 96 weeks after switching to a DOR-based regimen, possibly representing the background rate for these events. This suggests that DOR-based therapy may be a good option for adults with baseline neuropsychiatric symptoms or those experiencing NPAEs with other antiretrovirals.
期刊介绍:
JAIDS: Journal of Acquired Immune Deficiency Syndromes seeks to end the HIV epidemic by presenting important new science across all disciplines that advance our understanding of the biology, treatment and prevention of HIV infection worldwide.
JAIDS: Journal of Acquired Immune Deficiency Syndromes is the trusted, interdisciplinary resource for HIV- and AIDS-related information with a strong focus on basic and translational science, clinical science, and epidemiology and prevention. Co-edited by the foremost leaders in clinical virology, molecular biology, and epidemiology, JAIDS publishes vital information on the advances in diagnosis and treatment of HIV infections, as well as the latest research in the development of therapeutics and vaccine approaches. This ground-breaking journal brings together rigorously peer-reviewed articles, reviews of current research, results of clinical trials, and epidemiologic reports from around the world.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


