{"title":"Analysis of Clinical Symptoms and Risk Factors Related to Functional Prognosis in Patients With Cardiogenic Stroke.","authors":"Pen-Ju Liu, Shui-Ping Liu, Peng Yuan","doi":"10.14503/THIJ-24-8428","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiogenic stroke is associated with substantial morbidity and mortality, necessitating a better understanding of its clinical characteristics for improved patient outcomes. This study aimed to identify clinical characteristics influencing short-term functional prognosis in patients with cardiogenic stroke.</p><p><strong>Methods: </strong>The study prospectively enrolled 212 patients with cardiogenic stroke, collecting their clinical data and laboratory results. The modified Rankin Scale score at 90 days was used to define functional prognosis, with patients having a good prognosis (modified Rankin Scale ≤2; n = 164) or poor prognosis (modified Rankin Scale ≥3; n = 48).</p><p><strong>Results: </strong>The poor prognosis group had higher rates of total anterior circulation infarcts (12.5% vs 0.0%; <i>P</i> < .001) and posterior circulation infarction (50.0% vs 38.4%; <i>P</i> < .001) compared with the good prognosis group. Lesion characteristics differed significantly, with the poor prognosis group exhibiting more large-area lesions (39.6% vs 18.9%; <i>P</i> < .001) and multiple confluent lesions (56.3% vs 24.4%; <i>P</i> < .001). Admission-based National Institute of Health Stroke Scale scores were higher in the poor prognosis group (median [IQR], 12 [8-18] vs 5 [4-7]; <i>P</i> <.001), correlating with worse outcomes. The admission National Institute of Health Stroke Scale score predicted patients' 90-day prognosis with good accuracy (area under the curve, 0.937 [95% CI, 0.895-0.965]; <i>P</i> < .001), with a threshold of 7 yielding 85.42% sensitivity and 85.37% specificity.</p><p><strong>Conclusion: </strong>Higher admission National Institute of Health Stroke Scale scores were significantly associated with poor functional prognosis at 90 days, highlighting the importance of early National Institute of Health Stroke Scale-based assessment for improved outcomes.</p>","PeriodicalId":48680,"journal":{"name":"Texas Heart Institute Journal","volume":"51 2","pages":"e248428"},"PeriodicalIF":0.9000,"publicationDate":"2024-12-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11666877/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Texas Heart Institute Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14503/THIJ-24-8428","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cardiogenic stroke is associated with substantial morbidity and mortality, necessitating a better understanding of its clinical characteristics for improved patient outcomes. This study aimed to identify clinical characteristics influencing short-term functional prognosis in patients with cardiogenic stroke.
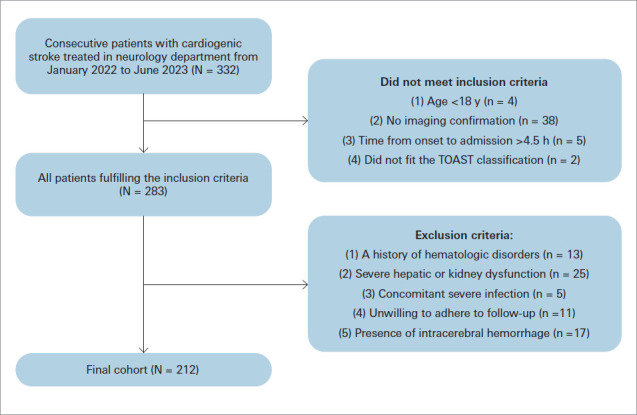
Methods: The study prospectively enrolled 212 patients with cardiogenic stroke, collecting their clinical data and laboratory results. The modified Rankin Scale score at 90 days was used to define functional prognosis, with patients having a good prognosis (modified Rankin Scale ≤2; n = 164) or poor prognosis (modified Rankin Scale ≥3; n = 48).
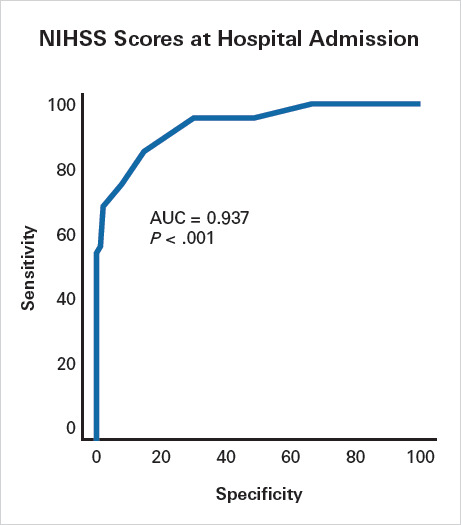
Results: The poor prognosis group had higher rates of total anterior circulation infarcts (12.5% vs 0.0%; P < .001) and posterior circulation infarction (50.0% vs 38.4%; P < .001) compared with the good prognosis group. Lesion characteristics differed significantly, with the poor prognosis group exhibiting more large-area lesions (39.6% vs 18.9%; P < .001) and multiple confluent lesions (56.3% vs 24.4%; P < .001). Admission-based National Institute of Health Stroke Scale scores were higher in the poor prognosis group (median [IQR], 12 [8-18] vs 5 [4-7]; P <.001), correlating with worse outcomes. The admission National Institute of Health Stroke Scale score predicted patients' 90-day prognosis with good accuracy (area under the curve, 0.937 [95% CI, 0.895-0.965]; P < .001), with a threshold of 7 yielding 85.42% sensitivity and 85.37% specificity.
Conclusion: Higher admission National Institute of Health Stroke Scale scores were significantly associated with poor functional prognosis at 90 days, highlighting the importance of early National Institute of Health Stroke Scale-based assessment for improved outcomes.
期刊介绍:
For more than 45 years, the Texas Heart Institute Journal has been published by the Texas Heart Institute as part of its medical education program. Our bimonthly peer-reviewed journal enjoys a global audience of physicians, scientists, and healthcare professionals who are contributing to the prevention, diagnosis, and treatment of cardiovascular disease.
The Journal was printed under the name of Cardiovascular Diseases from 1974 through 1981 (ISSN 0093-3546). The name was changed to Texas Heart Institute Journal in 1982 and was printed through 2013 (ISSN 0730-2347). In 2014, the Journal moved to online-only publication. It is indexed by Index Medicus/MEDLINE and by other indexing and abstracting services worldwide. Our full archive is available at PubMed Central.
The Journal invites authors to submit these article types for review:
-Clinical Investigations-
Laboratory Investigations-
Reviews-
Techniques-
Coronary Anomalies-
History of Medicine-
Case Reports/Case Series (Submission Fee: $70.00 USD)-
Images in Cardiovascular Medicine (Submission Fee: $35.00 USD)-
Guest Editorials-
Peabody’s Corner-
Letters to the Editor

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


