Prachi Bhatt, Jared Hirsch, Paul Cockrum, George Kim, Gabriela Dieguez
{"title":"The Effects of Adverse Events and Associated Costs on Value-Based Care for Metastatic Pancreatic Ductal Adenocarcinoma.","authors":"Prachi Bhatt, Jared Hirsch, Paul Cockrum, George Kim, Gabriela Dieguez","doi":"10.36469/001c.124367","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Rising oncology healthcare costs have led to value-based care reimbursement models that coordinate care and improve quality while reducing overall spending. These models are increasingly important for traditional Medicare and other payers. <b>Objectives:</b> To compare the incidence of adverse events (AEs), AE-associated excess costs, and total cost of care (TCOC) of 3 cohorts receiving first-line treatment for metastatic pancreatic ductal adenocarcinoma (mPDAC). <b>Methods:</b> We conducted a retrospective analysis of administrative claims data from 2018 to 2022 using the Medicare 100% Research Identifiable Files. We examined 3 cohorts receiving mPDAC treatment: FOLFIRINOX (FFX) (oxaliplatin, irinotecan, leucovorin, 5-FU bolus and infusion); modified FFX, (5-FU infusion only); and gemcitabine/nab-paclitaxel (gem/abrax). We compared the incidence of clinically significant AEs, TCOC, components of TCOC, and costs related to AEs/treatment toxicity. <b>Results:</b> Patient AE rates ranged from 6.2% to 51.7%. AEs occurred more frequently in patients receiving FFX with all 4 components. Patients receiving brand name gem/abrax had lower rates of febrile neutropenia (6.2%) and neutropenia (22.2%) than those receiving FFX with no 5-FU bolus (febrile neutropenia, 9.9%; neutropenia, 36.9%) and FFX with all 4 components (febrile neutropenia, 6.9%; neutropenia, 30.4%). Rates of most nonhematologic AEs were higher in patients receiving FFX with all 4 components, with diarrhea occurring in 28.3%, abdominal pain in 31.5%, and nausea/vomiting in 41.5% of patients. TCOC was lower in the gem/abrax cohort: <math><mn>6505</mn> <mi>v</mi> <mi>s</mi> <mi>F</mi> <mi>F</mi> <mi>X</mi> <mi>w</mi> <mi>i</mi> <mi>t</mi> <mi>h</mi> <mi>n</mi> <mi>o</mi> <mn>5</mn> <mo>-</mo> <mi>F</mi> <mi>U</mi> <mi>b</mi> <mi>o</mi> <mi>l</mi> <mi>u</mi> <mi>s</mi> <mo>(</mo></math> 6995) and FFX with all 4 components ( <math><mn>7142</mn> <mo>)</mo> <mi>p</mi> <mi>e</mi> <mi>r</mi> <mi>a</mi> <mi>d</mi> <mi>m</mi> <mi>i</mi> <mi>n</mi> <mi>i</mi> <mi>s</mi> <mi>t</mi> <mi>r</mi> <mi>a</mi> <mi>t</mi> <mi>i</mi> <mi>o</mi> <mi>n</mi> <mo>.</mo> <mi>T</mi> <mi>h</mi> <mi>e</mi> <mi>d</mi> <mi>e</mi> <mi>v</mi> <mi>e</mi> <mi>l</mi> <mi>o</mi> <mi>p</mi> <mi>m</mi> <mi>e</mi> <mi>n</mi> <mi>t</mi> <mi>o</mi> <mi>f</mi> <mi>a</mi> <mi>n</mi> <mi>y</mi> <mi>s</mi> <mi>t</mi> <mi>u</mi> <mi>d</mi> <mi>i</mi> <mi>e</mi> <mi>d</mi> <mi>h</mi> <mi>e</mi> <mi>m</mi> <mi>a</mi> <mi>t</mi> <mi>o</mi> <mi>l</mi> <mi>o</mi> <mi>g</mi> <mi>i</mi> <mi>c</mi> <mi>A</mi> <mi>E</mi> <mi>w</mi> <mi>a</mi> <mi>s</mi> <mi>a</mi> <mi>s</mi> <mi>s</mi> <mi>o</mi> <mi>c</mi> <mi>i</mi> <mi>a</mi> <mi>t</mi> <mi>e</mi> <mi>d</mi> <mi>w</mi> <mi>i</mi> <mi>t</mi> <mi>h</mi> <mi>a</mi> <mi>m</mi> <mi>e</mi> <mi>a</mi> <mi>n</mi> <mi>e</mi> <mi>x</mi> <mi>c</mi> <mi>e</mi> <mi>s</mi> <mi>s</mi> <mi>c</mi> <mi>o</mi> <mi>s</mi> <mi>t</mi> <mi>o</mi> <mi>f</mi></math> 5993 per administration, while the development of any studied nonhematological AE was associated with a mean per-administration excess cost of $3665. <b>Discussion:</b> Treatment decisions intended to minimize chemotherapy costs may lead to suboptimal decisions if the goal is to reduce TCOC. Our research suggests FFX is more costly than gem/abrax (TCOC per administration). Patients receiving gem/abrax were older and had higher baseline Charlson Comorbidity Index scores; however, other factors may be important in driving cost differences. <b>Conclusions:</b> Irrespective of drug cost, chemotherapy leading to a significant increase in AEs is associated with higher TCOC.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"11 2","pages":"161-167"},"PeriodicalIF":2.3000,"publicationDate":"2024-12-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11664866/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36469/001c.124367","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
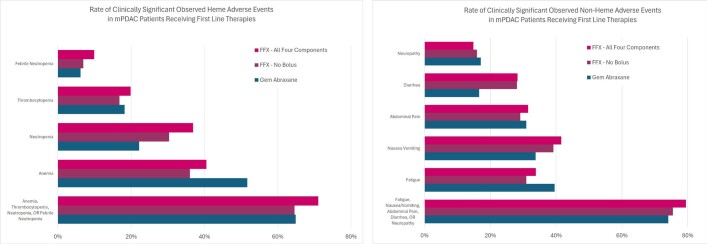
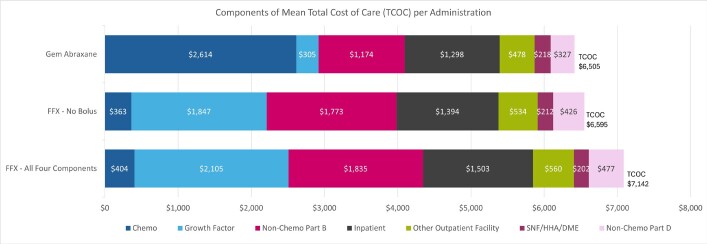
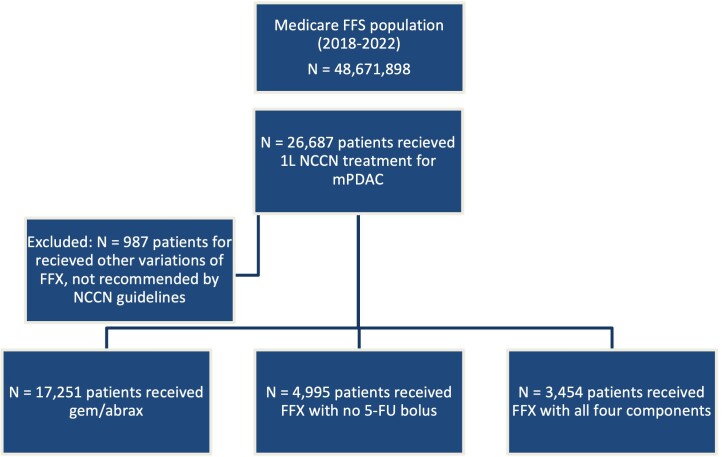
Background: Rising oncology healthcare costs have led to value-based care reimbursement models that coordinate care and improve quality while reducing overall spending. These models are increasingly important for traditional Medicare and other payers. Objectives: To compare the incidence of adverse events (AEs), AE-associated excess costs, and total cost of care (TCOC) of 3 cohorts receiving first-line treatment for metastatic pancreatic ductal adenocarcinoma (mPDAC). Methods: We conducted a retrospective analysis of administrative claims data from 2018 to 2022 using the Medicare 100% Research Identifiable Files. We examined 3 cohorts receiving mPDAC treatment: FOLFIRINOX (FFX) (oxaliplatin, irinotecan, leucovorin, 5-FU bolus and infusion); modified FFX, (5-FU infusion only); and gemcitabine/nab-paclitaxel (gem/abrax). We compared the incidence of clinically significant AEs, TCOC, components of TCOC, and costs related to AEs/treatment toxicity. Results: Patient AE rates ranged from 6.2% to 51.7%. AEs occurred more frequently in patients receiving FFX with all 4 components. Patients receiving brand name gem/abrax had lower rates of febrile neutropenia (6.2%) and neutropenia (22.2%) than those receiving FFX with no 5-FU bolus (febrile neutropenia, 9.9%; neutropenia, 36.9%) and FFX with all 4 components (febrile neutropenia, 6.9%; neutropenia, 30.4%). Rates of most nonhematologic AEs were higher in patients receiving FFX with all 4 components, with diarrhea occurring in 28.3%, abdominal pain in 31.5%, and nausea/vomiting in 41.5% of patients. TCOC was lower in the gem/abrax cohort: 6995) and FFX with all 4 components ( 5993 per administration, while the development of any studied nonhematological AE was associated with a mean per-administration excess cost of $3665. Discussion: Treatment decisions intended to minimize chemotherapy costs may lead to suboptimal decisions if the goal is to reduce TCOC. Our research suggests FFX is more costly than gem/abrax (TCOC per administration). Patients receiving gem/abrax were older and had higher baseline Charlson Comorbidity Index scores; however, other factors may be important in driving cost differences. Conclusions: Irrespective of drug cost, chemotherapy leading to a significant increase in AEs is associated with higher TCOC.
背景:不断上升的肿瘤医疗保健费用导致了基于价值的护理报销模式,协调护理和提高质量,同时减少总体支出。这些模式对传统医疗保险和其他支付者越来越重要。目的:比较3个队列接受转移性胰腺导管腺癌(mPDAC)一线治疗的不良事件(ae)发生率、ae相关的超额费用和总护理成本(TCOC)。方法:我们使用医疗保险100%研究可识别文件对2018年至2022年的行政索赔数据进行回顾性分析。我们检查了3个接受mPDAC治疗的队列:FOLFIRINOX (FFX)(奥沙利铂、伊立替康、亚叶酸素、5-FU丸和输注);改良的FFX(仅5-FU输注);吉西他滨/nab-紫杉醇(gem/abrax)。我们比较了临床显著ae的发生率、TCOC、TCOC成分以及与ae /治疗毒性相关的费用。结果:AE发生率为6.2% ~ 51.7%。所有4种成分均接受FFX治疗的患者发生不良事件的频率更高。接受gem/abrax品牌治疗的患者发热性中性粒细胞减少率(6.2%)和中性粒细胞减少率(22.2%)低于接受FFX治疗但不服用5-FU的患者(发热性中性粒细胞减少,9.9%;中性粒细胞减少症,36.9%)和所有4种成分的FFX(发热性中性粒细胞减少症,6.9%;嗜中性白血球减少症,30.4%)。所有4种成分均接受FFX治疗的患者中,大多数非血液学不良事件发生率较高,其中腹泻发生率为28.3%,腹痛发生率为31.5%,恶心/呕吐发生率为41.5%。TCOC较低的宝石/ abrax群:6505 v s F F X w i t h n o 5 - F U l b o s(6995)和FFX所有4组件(7142)p e r d m我n s t r t i o n。T h e d e v e l o p m e n T o f n y s T u i e d h e m T o d l o g i c a e w s s s o c i T e d w i T h m e n e x c e s s c o s T o f 5993 /政府,而任何的发展研究nonhematological AE与平均per-administration超过3665美元的成本。讨论:如果目标是降低TCOC,以最小化化疗费用为目的的治疗决策可能导致次优决策。我们的研究表明,FFX比gem/abrax更昂贵(每次给药的TCOC)。接受gem/abrax治疗的患者年龄较大,基线Charlson合并症指数评分较高;然而,在造成成本差异方面,其他因素可能也很重要。结论:无论药物成本如何,化疗导致ae显著增加与较高的TCOC相关。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


