Jordan M Cloyd, Rakhsha Khatri, Angela Sarna, Lena Stevens, Victor Heh, Mary Dillhoff, Alex Kim, Timothy M Pawlik, Aslam Ejaz, Sharla Wells-Di Gregorio, Erin Scott, Sachin S Kale
{"title":"Early Palliative Care Following Aborted Cancer Surgery: Results of a Prospective Feasibility Trial.","authors":"Jordan M Cloyd, Rakhsha Khatri, Angela Sarna, Lena Stevens, Victor Heh, Mary Dillhoff, Alex Kim, Timothy M Pawlik, Aslam Ejaz, Sharla Wells-Di Gregorio, Erin Scott, Sachin S Kale","doi":"10.1097/AS9.0000000000000520","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Although resection is generally necessary for curative-intent treatment of most solid organ cancers, surgery is occasionally aborted due to intraoperative findings. Following aborted cancer surgery, patients have unique care needs that specialized palliative care (PC) providers may be best equipped to manage. We hypothesized that early ambulatory PC referral following aborted cancer surgery would be feasible and acceptable.</p><p><strong>Methods: </strong>This single-institution prospective clinical trial enrolled adult patients with gastrointestinal or hepatopancreatobiliary cancer with no prior PC exposure who had curative-intent oncologic surgery that was unexpectedly aborted. The primary endpoint was the completion of an ambulatory PC consultation within 30 days of enrollment. Secondary outcomes included changes in standardized measures of quality-of-life (QOL) and anxiety/depression during the 3-month follow-up.</p><p><strong>Results: </strong>Among 25 enrolled participants, the mean age was 65.3 ± 9.9 years, 68% were male, and 88% were White. The most common types of cancers were pancreatic (44%), hepatobiliary (20%), and colorectal (12%); reasons for aborting surgery were occult metastatic disease (52%) and local unresectability (36%). Only 13 of 25 (52%) met the primary endpoint of ambulatory PC within 30 days, less than the prespecified threshold of 70%. Overall, 16 (64%) patients completed ambulatory PC consultation a mean of 29.2 ± 15.8 days after enrollment. Of the 9 (36%) who did not, reasons included patient preference (n = 4), withdrawal from study (n = 1), lost to follow-up (n = 1), scheduling conflict (n = 1), and required inpatient PC before discharge (n = 2). Anxiety (4.94 ± 3.56 vs 3.35 ± 2.60, <i>P</i> = 0.06), depression (4.18 ± 4.02 vs 4.76 ± 3.44, <i>P</i> = 0.49), and QOL (82.44 ± 11.41 vs 82.03 ± 15.37, <i>P</i> = 0.92) scores did not significantly differ at 3-month follow-up compared to baseline.</p><p><strong>Conclusions: </strong>Barriers to early ambulatory palliative care consultation exist after aborted cancer surgery. Given the unique and complex care needs of this patient population, additional research is needed to optimize supportive care strategies.</p>","PeriodicalId":72231,"journal":{"name":"Annals of surgery open : perspectives of surgical history, education, and clinical approaches","volume":"5 4","pages":"e520"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11661761/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of surgery open : perspectives of surgical history, education, and clinical approaches","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/AS9.0000000000000520","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Although resection is generally necessary for curative-intent treatment of most solid organ cancers, surgery is occasionally aborted due to intraoperative findings. Following aborted cancer surgery, patients have unique care needs that specialized palliative care (PC) providers may be best equipped to manage. We hypothesized that early ambulatory PC referral following aborted cancer surgery would be feasible and acceptable.
Methods: This single-institution prospective clinical trial enrolled adult patients with gastrointestinal or hepatopancreatobiliary cancer with no prior PC exposure who had curative-intent oncologic surgery that was unexpectedly aborted. The primary endpoint was the completion of an ambulatory PC consultation within 30 days of enrollment. Secondary outcomes included changes in standardized measures of quality-of-life (QOL) and anxiety/depression during the 3-month follow-up.
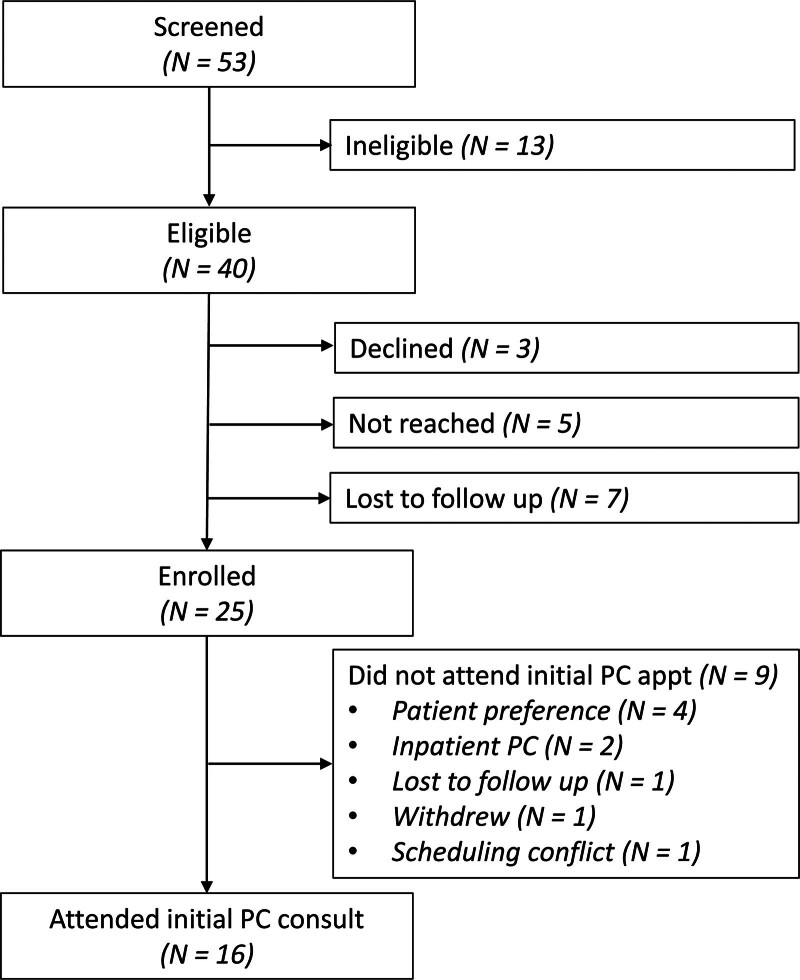
Results: Among 25 enrolled participants, the mean age was 65.3 ± 9.9 years, 68% were male, and 88% were White. The most common types of cancers were pancreatic (44%), hepatobiliary (20%), and colorectal (12%); reasons for aborting surgery were occult metastatic disease (52%) and local unresectability (36%). Only 13 of 25 (52%) met the primary endpoint of ambulatory PC within 30 days, less than the prespecified threshold of 70%. Overall, 16 (64%) patients completed ambulatory PC consultation a mean of 29.2 ± 15.8 days after enrollment. Of the 9 (36%) who did not, reasons included patient preference (n = 4), withdrawal from study (n = 1), lost to follow-up (n = 1), scheduling conflict (n = 1), and required inpatient PC before discharge (n = 2). Anxiety (4.94 ± 3.56 vs 3.35 ± 2.60, P = 0.06), depression (4.18 ± 4.02 vs 4.76 ± 3.44, P = 0.49), and QOL (82.44 ± 11.41 vs 82.03 ± 15.37, P = 0.92) scores did not significantly differ at 3-month follow-up compared to baseline.
Conclusions: Barriers to early ambulatory palliative care consultation exist after aborted cancer surgery. Given the unique and complex care needs of this patient population, additional research is needed to optimize supportive care strategies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


