Gabriela Pilz da Cunha, Jasper P Sijberden, Susan van Dieren, Paul Gobardhan, Daan J Lips, Türkan Terkivatan, Hendrik A Marsman, Gijs A Patijn, Wouter K G Leclercq, Koop Bosscha, J Sven D Mieog, Peter B van den Boezem, Maarten Vermaas, Niels F M Kok, Eric J T Belt, Marieke T de Boer, Wouter J M Derksen, Hans Torrenga, Paul M Verheijen, Steven J Oosterling, Arjen M Rijken, Marielle M E Coolsen, Mike S L Liem, T C Khé Tran, Michael F Gerhards, Vincent Nieuwenhuijs, Mohammad Abu Hilal, Marc G Besselink, Ronald M van Dam, Jeroen Hagendoorn, Rutger-Jan Swijnenburg
{"title":"Robotic Versus Laparoscopic Liver Resection: A Nationwide Propensity Score Matched Analysis.","authors":"Gabriela Pilz da Cunha, Jasper P Sijberden, Susan van Dieren, Paul Gobardhan, Daan J Lips, Türkan Terkivatan, Hendrik A Marsman, Gijs A Patijn, Wouter K G Leclercq, Koop Bosscha, J Sven D Mieog, Peter B van den Boezem, Maarten Vermaas, Niels F M Kok, Eric J T Belt, Marieke T de Boer, Wouter J M Derksen, Hans Torrenga, Paul M Verheijen, Steven J Oosterling, Arjen M Rijken, Marielle M E Coolsen, Mike S L Liem, T C Khé Tran, Michael F Gerhards, Vincent Nieuwenhuijs, Mohammad Abu Hilal, Marc G Besselink, Ronald M van Dam, Jeroen Hagendoorn, Rutger-Jan Swijnenburg","doi":"10.1097/AS9.0000000000000527","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To compare nationwide outcomes of robotic liver resection (RLR) with laparoscopic liver resection (LLR).</p><p><strong>Background: </strong>Minimally invasive liver resection is increasingly performed using the robotic approach as this could help overcome inherent technical limitations of laparoscopy. It is unknown if this translates to improved patient outcomes.</p><p><strong>Methods: </strong>Data from the mandatory Dutch Hepatobiliary Audit were used to compare perioperative outcomes of RLR and LLR in 20 centers in the Netherlands (2014-2022). Propensity score matching (PSM) was used to mitigate selection bias. Sensitivity analyses assessed the impact of the learning curve (≥50 procedures for LLR and ≥25 procedures for RLR), concurrent noncholecystectomy operations, high-volume centers, and conversion on outcomes.</p><p><strong>Results: </strong>Overall, 792 RLR and 2738 LLR were included. After PSM (781 RLR vs 781 LLR), RLR was associated with less blood loss (median: 100 mL [interquartile range (IQR): 50-300] vs 200 mL [IQR: 50-500], <i>P</i> = 0.002), less major blood loss (≥500 mL,18.6% vs 25.2%, <i>P</i> = 0.011), less conversions (4.9% vs 12.8%, <i>P</i> < 0.001), and shorter hospital stay (median: 3 days [IQR: 2-5] vs 4 days [IQR: 2-6], <i>P</i> < 0.001), compared with LLR. There were no significant differences in overall and severe morbidity, readmissions, mortality, and R0 resection rate. Sensitivity analyses yielded similar results. When excluding conversions, RLR was only associated with a reduction in reoperations (1.1% vs 2.7%, <i>P</i> = 0.038).</p><p><strong>Conclusion: </strong>In this nationwide analysis, RLR was associated with a reduction in conversion, blood loss and length of hospital stay without compromising patient safety, also when excluding a learning curve effect. The benefits of RLR seem to be mostly related to a reduction in conversions.</p>","PeriodicalId":72231,"journal":{"name":"Annals of surgery open : perspectives of surgical history, education, and clinical approaches","volume":"5 4","pages":"e527"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11661729/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of surgery open : perspectives of surgical history, education, and clinical approaches","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/AS9.0000000000000527","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To compare nationwide outcomes of robotic liver resection (RLR) with laparoscopic liver resection (LLR).
Background: Minimally invasive liver resection is increasingly performed using the robotic approach as this could help overcome inherent technical limitations of laparoscopy. It is unknown if this translates to improved patient outcomes.
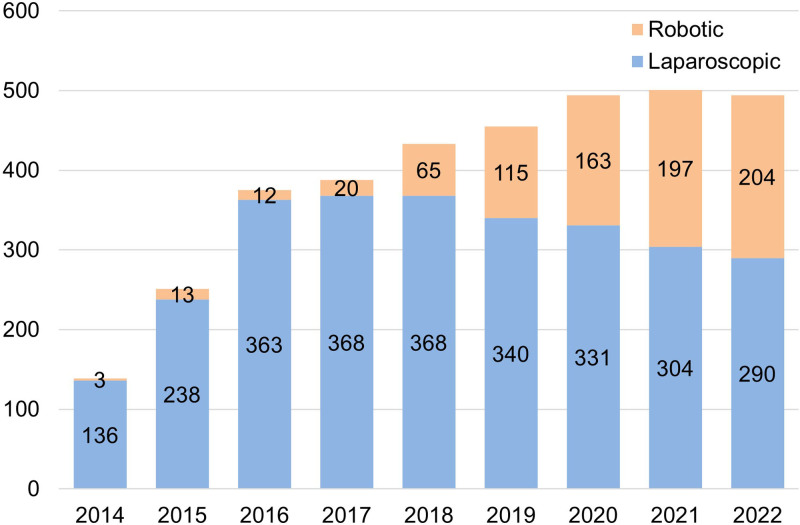
Methods: Data from the mandatory Dutch Hepatobiliary Audit were used to compare perioperative outcomes of RLR and LLR in 20 centers in the Netherlands (2014-2022). Propensity score matching (PSM) was used to mitigate selection bias. Sensitivity analyses assessed the impact of the learning curve (≥50 procedures for LLR and ≥25 procedures for RLR), concurrent noncholecystectomy operations, high-volume centers, and conversion on outcomes.
Results: Overall, 792 RLR and 2738 LLR were included. After PSM (781 RLR vs 781 LLR), RLR was associated with less blood loss (median: 100 mL [interquartile range (IQR): 50-300] vs 200 mL [IQR: 50-500], P = 0.002), less major blood loss (≥500 mL,18.6% vs 25.2%, P = 0.011), less conversions (4.9% vs 12.8%, P < 0.001), and shorter hospital stay (median: 3 days [IQR: 2-5] vs 4 days [IQR: 2-6], P < 0.001), compared with LLR. There were no significant differences in overall and severe morbidity, readmissions, mortality, and R0 resection rate. Sensitivity analyses yielded similar results. When excluding conversions, RLR was only associated with a reduction in reoperations (1.1% vs 2.7%, P = 0.038).
Conclusion: In this nationwide analysis, RLR was associated with a reduction in conversion, blood loss and length of hospital stay without compromising patient safety, also when excluding a learning curve effect. The benefits of RLR seem to be mostly related to a reduction in conversions.
目的:比较全国范围内机器人肝切除术(RLR)与腹腔镜肝切除术(LLR)的效果。背景:微创肝切除术越来越多地采用机器人方法进行,因为这有助于克服腹腔镜固有的技术局限性。目前尚不清楚这是否会改善患者的预后。方法:采用强制性荷兰肝胆审计的数据,比较荷兰20个中心(2014-2022年)RLR和LLR的围手术期结果。倾向得分匹配(PSM)用于减轻选择偏差。敏感性分析评估了学习曲线(LLR≥50例,RLR≥25例)、同期非胆囊切除术、大容量中心和转换对结果的影响。结果:共纳入RLR 792例,LLR 2738例。PSM (781 RLR vs 781 LLR)后,与LLR相比,RLR与更少的失血量(中位数:100 mL[四分位间距(IQR): 50-300] vs 200 mL [IQR: 50-500], P = 0.002)、更少的主要失血量(≥500 mL,18.6% vs 25.2%, P = 0.011)、更少的转诊(4.9% vs 12.8%, P < 0.001)和更短的住院时间(中位数:3天[IQR: 2-5] vs 4天[IQR: 2-6], P < 0.001)相关。在总体和严重的发病率、再入院率、死亡率和R0切除率方面没有显著差异。敏感性分析得出了类似的结果。当排除转归时,RLR仅与再手术的减少相关(1.1% vs 2.7%, P = 0.038)。结论:在这项全国性的分析中,RLR与减少转换率、出血量和住院时间有关,而且在排除学习曲线效应的情况下,也不会影响患者的安全。RLR的好处似乎主要与转化率的降低有关。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


