Predictors of Recurrence After Curative Surgery for Stage I Colon Cancer: Retrospective Cohort Analysis of the Italian Society of Surgical Oncology Colorectal Cancer Network Collaborative Group.
Giulia Turri, Luigi Martinelli, Daniela Rega, Nicolò Tamini, Lucia Paiano, Simona Deidda, QuocRiccardo Bao, Laura Lorenzon, Raffaele De Luca, Caterina Foppa, Valentina Mari, Giovanni Taffurelli, Arcangelo Picciariello, Patrizia Marsanic, Leandro Siragusa, Francesco Bagolini, Riccardo Nascimbeni, Gianluca Rizzo, Sara Vertaldi, Michele Zuolo, Giorgio Bianchi, Lisa Marie Rorato, Rossella Reddavid, Gaetano Gallo, Lorenzo Crepaz, Alberto Di Leo, Mario Trompetto, Enrico Potenza, Mauro Santarelli, Nicola de'Angelis, Francesco Ciarleglio, Marco Milone, Claudio Coco, Guido Alberto Tiberio, Gabriele Anania, Giuseppe S Sica, Andrea Muratore, Donato Francesco Altomare, Isacco Montroni, Maurizio De Luca, Antonino Spinelli, Michele Simone, Roberto Persiani, Gaya Spolverato, Angelo Restivo, Nicolò de Manzini, Marco Braga, Paolo Delrio, Giuseppe Verlato, Corrado Pedrazzani
{"title":"Predictors of Recurrence After Curative Surgery for Stage I Colon Cancer: Retrospective Cohort Analysis of the Italian Society of Surgical Oncology Colorectal Cancer Network Collaborative Group.","authors":"Giulia Turri, Luigi Martinelli, Daniela Rega, Nicolò Tamini, Lucia Paiano, Simona Deidda, QuocRiccardo Bao, Laura Lorenzon, Raffaele De Luca, Caterina Foppa, Valentina Mari, Giovanni Taffurelli, Arcangelo Picciariello, Patrizia Marsanic, Leandro Siragusa, Francesco Bagolini, Riccardo Nascimbeni, Gianluca Rizzo, Sara Vertaldi, Michele Zuolo, Giorgio Bianchi, Lisa Marie Rorato, Rossella Reddavid, Gaetano Gallo, Lorenzo Crepaz, Alberto Di Leo, Mario Trompetto, Enrico Potenza, Mauro Santarelli, Nicola de'Angelis, Francesco Ciarleglio, Marco Milone, Claudio Coco, Guido Alberto Tiberio, Gabriele Anania, Giuseppe S Sica, Andrea Muratore, Donato Francesco Altomare, Isacco Montroni, Maurizio De Luca, Antonino Spinelli, Michele Simone, Roberto Persiani, Gaya Spolverato, Angelo Restivo, Nicolò de Manzini, Marco Braga, Paolo Delrio, Giuseppe Verlato, Corrado Pedrazzani","doi":"10.1097/AS9.0000000000000510","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The aim of this study is to provide solid evidence to update the management of stage I colon cancer (CC) after surgery.</p><p><strong>Background: </strong>Given the low risk of recurrence of stage I CC, some international guidelines do not recommend intensive follow-up after surgery. However, data on the actual incidence, risk factors, and site of recurrences are scarce.</p><p><strong>Methods: </strong>This is a retrospective multicenter cohort study considering patients who underwent surgery at 25 Italian centers between 2010 and 2019, with a minimum follow-up of 24 months. A total of 1883 consecutive adult patients with stage I CC treated with curative surgery were considered, and 1611 fulfilled the inclusion criteria. The primary outcome was the rate of recurrence. Secondary outcomes included survival and risk factors for recurrence.</p><p><strong>Results: </strong>Eighty patients developed cancer recurrence (5.0%), of which 90% was systemic relapse. The event was more frequent in pT2 (6.0% vs 3.2%, <i>P</i> = 0.013), male patients (6.1% vs 3.6%, <i>P</i> = 0.021), in the presence of lymphovascular invasion (7.2% vs 3.6%, <i>P</i> = 0.01), and in cases of partial resection (11.1% vs 4.6%, <i>P</i> = 0.011). Also, preoperative carcinoembryonic antigen (<i>P</i> = 0.007) and tumor diameter (<i>P</i> < 0.001) were higher in the group who relapsed. Most patients had isolated cancer recurrence (90%). Recurrences peaked between 10 and 18 months after surgery and declined over time. Adjusted Cox regression analysis identified tumor diameter, carcinoembryonic antigen level, lymphovascular invasion, male gender, and less than 12 analyzed lymph nodes as significant risk factors for worse recurrence-free survival.</p><p><strong>Conclusions: </strong>This study showed that a not negligible rate of stage I CC recur after curative surgery. Most relapses occur at a single site within the first 3 years after surgery. This evidence could be used to optimize postoperative follow-up.</p>","PeriodicalId":72231,"journal":{"name":"Annals of surgery open : perspectives of surgical history, education, and clinical approaches","volume":"5 4","pages":"e510"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11661724/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of surgery open : perspectives of surgical history, education, and clinical approaches","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/AS9.0000000000000510","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The aim of this study is to provide solid evidence to update the management of stage I colon cancer (CC) after surgery.
Background: Given the low risk of recurrence of stage I CC, some international guidelines do not recommend intensive follow-up after surgery. However, data on the actual incidence, risk factors, and site of recurrences are scarce.
Methods: This is a retrospective multicenter cohort study considering patients who underwent surgery at 25 Italian centers between 2010 and 2019, with a minimum follow-up of 24 months. A total of 1883 consecutive adult patients with stage I CC treated with curative surgery were considered, and 1611 fulfilled the inclusion criteria. The primary outcome was the rate of recurrence. Secondary outcomes included survival and risk factors for recurrence.
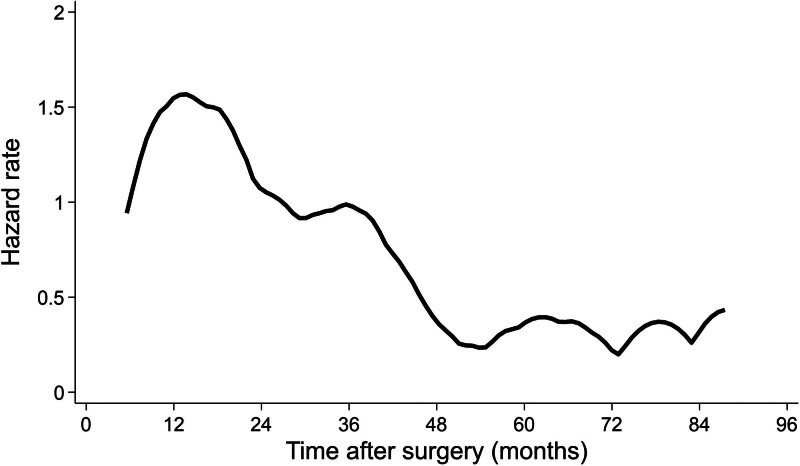
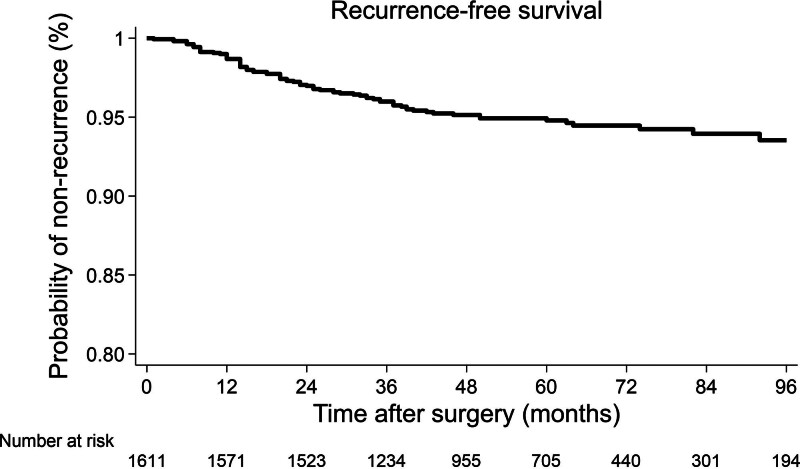
Results: Eighty patients developed cancer recurrence (5.0%), of which 90% was systemic relapse. The event was more frequent in pT2 (6.0% vs 3.2%, P = 0.013), male patients (6.1% vs 3.6%, P = 0.021), in the presence of lymphovascular invasion (7.2% vs 3.6%, P = 0.01), and in cases of partial resection (11.1% vs 4.6%, P = 0.011). Also, preoperative carcinoembryonic antigen (P = 0.007) and tumor diameter (P < 0.001) were higher in the group who relapsed. Most patients had isolated cancer recurrence (90%). Recurrences peaked between 10 and 18 months after surgery and declined over time. Adjusted Cox regression analysis identified tumor diameter, carcinoembryonic antigen level, lymphovascular invasion, male gender, and less than 12 analyzed lymph nodes as significant risk factors for worse recurrence-free survival.
Conclusions: This study showed that a not negligible rate of stage I CC recur after curative surgery. Most relapses occur at a single site within the first 3 years after surgery. This evidence could be used to optimize postoperative follow-up.
目的:本研究的目的是为更新一期结肠癌(CC)术后的管理提供可靠的证据。背景:考虑到I期CC的复发风险较低,一些国际指南不建议术后进行强化随访。然而,关于实际发病率、危险因素和复发部位的数据很少。方法:这是一项回顾性多中心队列研究,纳入了2010年至2019年在意大利25个中心接受手术的患者,随访时间至少为24个月。共纳入1883例连续接受根治性手术治疗的成年I期CC患者,其中1611例符合纳入标准。主要观察指标为复发率。次要结局包括生存和复发危险因素。结果:80例患者发生肿瘤复发(5.0%),其中90%为全身复发。pT2患者(6.0% vs 3.2%, P = 0.013)、男性患者(6.1% vs 3.6%, P = 0.021)、存在淋巴血管侵犯(7.2% vs 3.6%, P = 0.01)和部分切除患者(11.1% vs 4.6%, P = 0.011)的发生率更高。复发组术前癌胚抗原(P = 0.007)和肿瘤直径(P < 0.001)均高于复发组。大多数患者有孤立性癌症复发(90%)。复发率在手术后10至18个月达到顶峰,并随着时间的推移而下降。校正后的Cox回归分析发现,肿瘤直径、癌胚抗原水平、淋巴血管浸润、男性以及少于12例分析的淋巴结是导致无复发生存差的重要危险因素。结论:本研究显示一期CC术后复发率不可忽视。大多数复发发生在手术后的前3年内的一个部位。该证据可用于优化术后随访。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


