{"title":"Real-Time Fluorescence Imaging for Thoracic Duct Identification during Oesophagectomy: A Systematic Review of the Literature.","authors":"Dimitra V Peristeri, Minas Baltatzis","doi":"10.5090/jcs.24.091","DOIUrl":null,"url":null,"abstract":"<p><p>Postoperative chylothorax is a serious complication after oesophagectomy. Real-time identification of the thoracic duct (TD) could prevent injury or facilitate prompt management when it occurs. Intraoperative TD lymphography with indocyanine green (ICG) is a novel technique that may help prevent chyle leaks following thoracic surgery. A systematic search of PubMed, Embase, MEDLINE, Scopus, and the Cochrane Library for studies published until July 2024 evaluating ICG for TD identification during oesophagectomy was performed. Studies were included in the review if they assessed intraoperative TD identification with ICG to prevent chyle leakage in patients undergoing oesophagectomy. Nine of 265 screened papers were included in the present review, with 3 reporting comparative techniques of TD identification between patients. Only 1 study had a control group without ICG administration. TD was identified in 281 of the 303 patients who received ICG. Chyle leak incidence was 0.66% in the ICG group. The mean observation time of TD after ICG administration was 162 minutes. Most of the included patients received neoadjuvant treatment before surgery. Different application routes of ICG have been reported, with the most prominent one being through the inguinal region under ultrasound guidance. Real- time TD identification with ICG might be a valuable tool for avoiding injury or managing it intraoperatively. To our knowledge, this is the first systematic review on this complex topic. However, as no randomized controlled trials have been published, sufficient evidence is needed to determine whether the aforementioned method can sufficiently reduce the chyle leak rate.</p>","PeriodicalId":34499,"journal":{"name":"Journal of Chest Surgery","volume":" ","pages":"5-14"},"PeriodicalIF":1.0000,"publicationDate":"2025-01-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11738141/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Chest Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5090/jcs.24.091","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/23 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
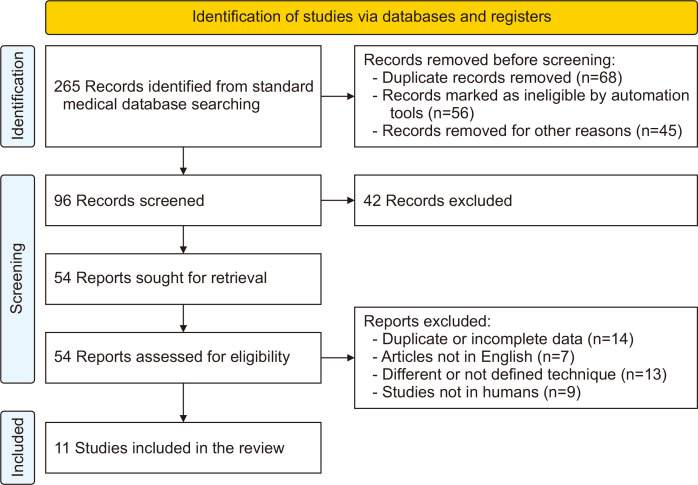
Postoperative chylothorax is a serious complication after oesophagectomy. Real-time identification of the thoracic duct (TD) could prevent injury or facilitate prompt management when it occurs. Intraoperative TD lymphography with indocyanine green (ICG) is a novel technique that may help prevent chyle leaks following thoracic surgery. A systematic search of PubMed, Embase, MEDLINE, Scopus, and the Cochrane Library for studies published until July 2024 evaluating ICG for TD identification during oesophagectomy was performed. Studies were included in the review if they assessed intraoperative TD identification with ICG to prevent chyle leakage in patients undergoing oesophagectomy. Nine of 265 screened papers were included in the present review, with 3 reporting comparative techniques of TD identification between patients. Only 1 study had a control group without ICG administration. TD was identified in 281 of the 303 patients who received ICG. Chyle leak incidence was 0.66% in the ICG group. The mean observation time of TD after ICG administration was 162 minutes. Most of the included patients received neoadjuvant treatment before surgery. Different application routes of ICG have been reported, with the most prominent one being through the inguinal region under ultrasound guidance. Real- time TD identification with ICG might be a valuable tool for avoiding injury or managing it intraoperatively. To our knowledge, this is the first systematic review on this complex topic. However, as no randomized controlled trials have been published, sufficient evidence is needed to determine whether the aforementioned method can sufficiently reduce the chyle leak rate.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


