Plasma Viral Load of 200 Copies/mL is a Suitable Threshold to Define Viral Suppression and HIV Drug Resistance Testing in Low- and Middle-Income Countries: Evidence From a Facility-Based Study in Cameroon.
Collins Ambe Chenwi, Rachel Audrey Nayang Mundo, Alex Durand Nka, Ezechiel Ngoufack Jagni Semengue, Grâce Angong Beloumou, Aude Christelle Ka'e, Willy Leroi Togna Pabo, Désiré Takou, Aissatou Abba, Sandrine Claire Djupsa, Evariste Molimbou, Naomi-Karell Etame, Aurelie Minelle Kengni Ngueko, David Kob Same, Jolle Nounouce Bouba Pamen, Aristide Stephane Abah Abah, Serge Clotaire Billong, Rogers Ajeh Awoh, Gregory Edie Halle-Ekane, Giulia Cappelli, Anne-Esther Njom-Nlend, Anne-Cecile Zk Bissek, Elvis Temfack, Maria Mercedes Santoro, Francesca Ceccherini-Silberstein, Vittorio Colizzi, Jean Kaseya, Nicaise Ndembi, Alexis Ndjolo, Carlo Federico Perno, Joseph Fokam
{"title":"Plasma Viral Load of 200 Copies/mL is a Suitable Threshold to Define Viral Suppression and HIV Drug Resistance Testing in Low- and Middle-Income Countries: Evidence From a Facility-Based Study in Cameroon.","authors":"Collins Ambe Chenwi, Rachel Audrey Nayang Mundo, Alex Durand Nka, Ezechiel Ngoufack Jagni Semengue, Grâce Angong Beloumou, Aude Christelle Ka'e, Willy Leroi Togna Pabo, Désiré Takou, Aissatou Abba, Sandrine Claire Djupsa, Evariste Molimbou, Naomi-Karell Etame, Aurelie Minelle Kengni Ngueko, David Kob Same, Jolle Nounouce Bouba Pamen, Aristide Stephane Abah Abah, Serge Clotaire Billong, Rogers Ajeh Awoh, Gregory Edie Halle-Ekane, Giulia Cappelli, Anne-Esther Njom-Nlend, Anne-Cecile Zk Bissek, Elvis Temfack, Maria Mercedes Santoro, Francesca Ceccherini-Silberstein, Vittorio Colizzi, Jean Kaseya, Nicaise Ndembi, Alexis Ndjolo, Carlo Federico Perno, Joseph Fokam","doi":"10.1177/23259582241306484","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>In low-and-middle-income-countries (LMIC), viral suppression is defined as plasma viral load (PVL) below 1000 copies/mL (low-level viremia [LLV]) and threshold for HIV drug resistance (HIVDR) testing. However, there is evidence that drug resistance mutations (DRMs) may emerge at LLV, thus compromising antiretroviral treatment (ART) response<b>.</b> We evaluated sequencing success rates (SSR) at LLV, described HIVDR profiles and adequacy with potential efficacy of tenofovir-lamivudine-dolutegravir (TLD).</p><p><strong>Methods: </strong>A cross-sectional study was conducted among individuals with LLV at the Chantal BIYA International Reference Centre, Yaoundé, Cameroon from January 2020 through August 2021. HIV-1 sequencing was performed on protease/reverse-transcriptase, and sequences analysed using Stanford HIVdbv9.5. SSR and HIVDR rates were assessed according to viral-load ranges, with <i>P</i> < .05 considered statistically significant.</p><p><strong>Results: </strong>In total, 131 individuals were enrolled (median [IQR] age = 41 [30-49] years; 67.9% female; 54.7% at WHO clinical-stage I/II; median ART-duration 7 [4-11] years; median CD4-count 221 [103-402] cells/mm<sup>3</sup> and median PVL 222 [96-436] copies/mL). Overall, SSR at LLV was 34.4% (45/131) and increased significantly with decreasing-age (<i>P = </i>.002) and increasing-PVL (<i>P </i>= .017). SSR were doubled at PVL≥150 copies/mL (21.8% at [40-150] vs. 43.3% at [150-1000]; OR = 2.8, <i>P = </i>.01). Of the 45 sequences obtained, 75.6% were recombinant strains (CRF02_AG, CRF09_cpx, CRF11_cpx) and 24.4% pure-subtypes (A1, D, F2, G). Overall, HIVDR prevalence at LLV was 82.2% (37/45), with 74.6% and 15.6% resistance to reverse-transcriptase inhibitors (RTIs) and ritonavir-boosted protease inhibitors (PI/r) respectively. Interestingly, HIVDR rates were similar at PVLs [50-200] versus [200-1000] copies/mL (<i>P = </i>.69). The most frequent DRMs were M184 V (73.3%) and K103N (40.0%) for RTIs and M46I (6.7%) for PIs/r. Overall 55.6% (25/45) of individuals were on suboptimal ART (needing ART-optimisation), with 48.9% (22/45) having suboptimal TLD predictive efficacy. Optimisation need was higher in first-line (81.8%, <i>P = </i>.03), but similar across viral clades and PVL-ranges (<i>P = </i>.6).</p><p><strong>Conclusion: </strong>In this LMIC context, sequencing for HIVDR is feasible at LLV even with broad HIV-1 diversity, with significantly higher SSR above 150 copies/mL and/or in paediatrics. About 80% of individuals with LLV harbour HIVDR strains, with half of them needing ART optimisations to limit HIVDR emergence and prevent treatment failure. Our findings underscore the clinical benefits of HIVDR during persisting LLV and the need to reconsider the threshold for viral suppression around 200copies/mL in LMICs.</p>","PeriodicalId":17328,"journal":{"name":"Journal of the International Association of Providers of AIDS Care","volume":"23 ","pages":"23259582241306484"},"PeriodicalIF":2.1000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11664513/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the International Association of Providers of AIDS Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23259582241306484","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: In low-and-middle-income-countries (LMIC), viral suppression is defined as plasma viral load (PVL) below 1000 copies/mL (low-level viremia [LLV]) and threshold for HIV drug resistance (HIVDR) testing. However, there is evidence that drug resistance mutations (DRMs) may emerge at LLV, thus compromising antiretroviral treatment (ART) response. We evaluated sequencing success rates (SSR) at LLV, described HIVDR profiles and adequacy with potential efficacy of tenofovir-lamivudine-dolutegravir (TLD).
Methods: A cross-sectional study was conducted among individuals with LLV at the Chantal BIYA International Reference Centre, Yaoundé, Cameroon from January 2020 through August 2021. HIV-1 sequencing was performed on protease/reverse-transcriptase, and sequences analysed using Stanford HIVdbv9.5. SSR and HIVDR rates were assessed according to viral-load ranges, with P < .05 considered statistically significant.
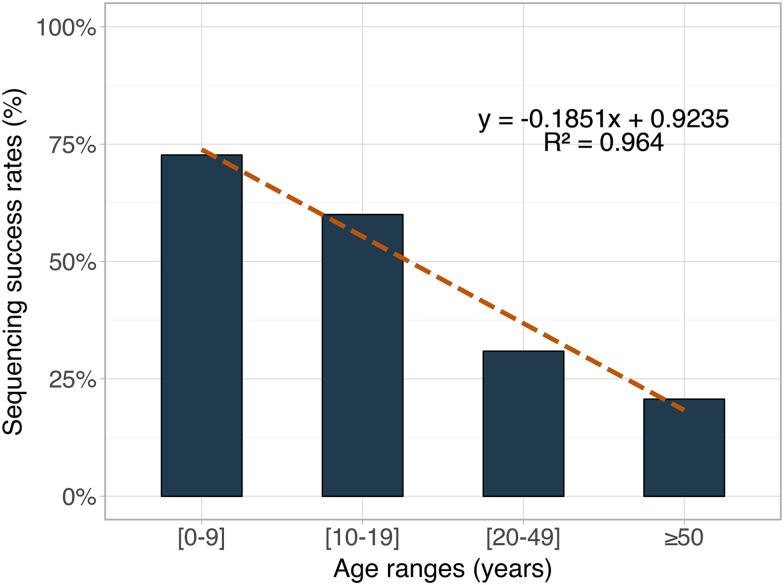
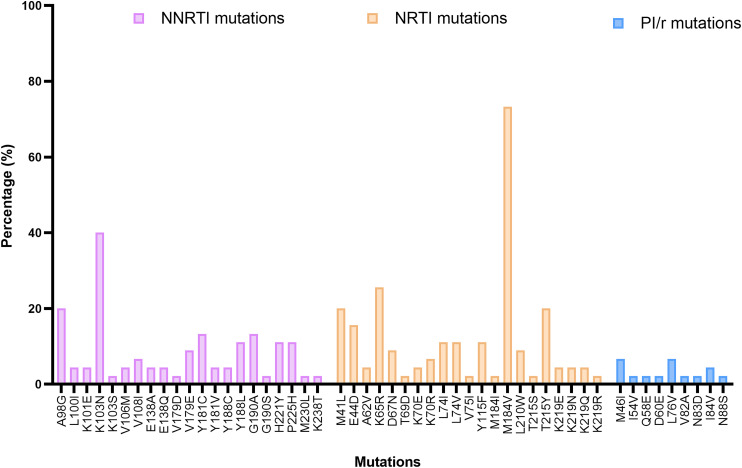
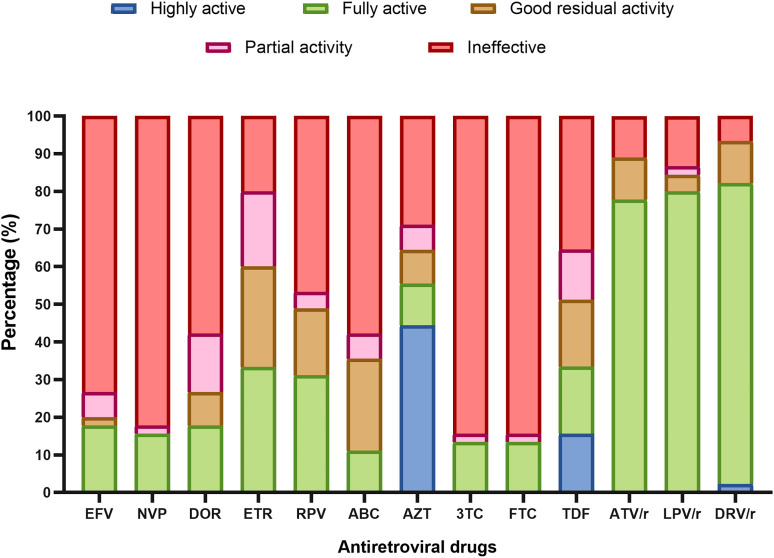
Results: In total, 131 individuals were enrolled (median [IQR] age = 41 [30-49] years; 67.9% female; 54.7% at WHO clinical-stage I/II; median ART-duration 7 [4-11] years; median CD4-count 221 [103-402] cells/mm3 and median PVL 222 [96-436] copies/mL). Overall, SSR at LLV was 34.4% (45/131) and increased significantly with decreasing-age (P = .002) and increasing-PVL (P = .017). SSR were doubled at PVL≥150 copies/mL (21.8% at [40-150] vs. 43.3% at [150-1000]; OR = 2.8, P = .01). Of the 45 sequences obtained, 75.6% were recombinant strains (CRF02_AG, CRF09_cpx, CRF11_cpx) and 24.4% pure-subtypes (A1, D, F2, G). Overall, HIVDR prevalence at LLV was 82.2% (37/45), with 74.6% and 15.6% resistance to reverse-transcriptase inhibitors (RTIs) and ritonavir-boosted protease inhibitors (PI/r) respectively. Interestingly, HIVDR rates were similar at PVLs [50-200] versus [200-1000] copies/mL (P = .69). The most frequent DRMs were M184 V (73.3%) and K103N (40.0%) for RTIs and M46I (6.7%) for PIs/r. Overall 55.6% (25/45) of individuals were on suboptimal ART (needing ART-optimisation), with 48.9% (22/45) having suboptimal TLD predictive efficacy. Optimisation need was higher in first-line (81.8%, P = .03), but similar across viral clades and PVL-ranges (P = .6).
Conclusion: In this LMIC context, sequencing for HIVDR is feasible at LLV even with broad HIV-1 diversity, with significantly higher SSR above 150 copies/mL and/or in paediatrics. About 80% of individuals with LLV harbour HIVDR strains, with half of them needing ART optimisations to limit HIVDR emergence and prevent treatment failure. Our findings underscore the clinical benefits of HIVDR during persisting LLV and the need to reconsider the threshold for viral suppression around 200copies/mL in LMICs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


