Socioeconomic Inequities in Preemptive Kidney Transplantation and Graft Survival: An Innovative Approach to Identifying Disparities in Kidney Transplantation.
Sarah Kizilbash, Chung-Ii Wi, Madison Roy, Euijung Ryu, Arthur Matas, Vesna Garovic, Samy Riad, Carrie Schinstock, Young Juhn
{"title":"Socioeconomic Inequities in Preemptive Kidney Transplantation and Graft Survival: An Innovative Approach to Identifying Disparities in Kidney Transplantation.","authors":"Sarah Kizilbash, Chung-Ii Wi, Madison Roy, Euijung Ryu, Arthur Matas, Vesna Garovic, Samy Riad, Carrie Schinstock, Young Juhn","doi":"10.1097/TXD.0000000000001734","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The limitations of conventional measures of socioeconomic status (SES) limit our ability to elucidate the role of SES as a key element of social determinants of health in kidney transplantation. This study's objective was to use an innovative SES measure, the HOUsing-based SES measure (HOUSES) index, to examine the effects of social determinants of health on access to and outcomes of kidney transplantation.</p><p><strong>Methods: </strong>Our study included residents of Minnesota (age older than 18 y) who underwent kidney transplantation at a single center between 2010 and 2020. SES was determined using the HOUSES index, categorized into quartiles (Q1 for lower, Q2-Q4 for higher SES). We used mixed-effects multivariable logistic and Cox models to examine the effects of HOUSES on preemptive transplants, pretransplant dialysis duration, and death-censored graft loss, adjusting for covariates.</p><p><strong>Results: </strong>Among 1975 eligible patients, 29.4% received preemptive transplants, 34.9% underwent pretransplant dialysis for >3 y, and 15.1% experienced death-censored graft loss for a median follow-up of 7.15 (interquartile range, 4.25-11.38) y. Lower SES recipients (Q1) demonstrated decreased preemptive transplant likelihood (adjusted odds ratio [aOR]: 0.74; 95% confidence interval [CI], 0.57-0.97; <i>P</i> = 0.03), longer dialysis duration (>3 y; aOR: 1.43; 95% CI, 1.01-2.03; <i>P</i> = 0.046), and higher death-censored graft loss (adjusted hazard ratio 1.36; 95% CI, 1.02-1.12; <i>P</i> = 0.036) versus higher SES recipients (Q2-Q4).</p><p><strong>Conclusions: </strong>We observed significant socioeconomic disparities in kidney transplant access, dialysis duration, and graft survival. The HOUSES index may be a promising tool for individual-based targeted interventions as it identifies SES on an individual rather than an area-level basis.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"11 1","pages":"e1734"},"PeriodicalIF":1.9000,"publicationDate":"2024-12-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11658720/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001734","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The limitations of conventional measures of socioeconomic status (SES) limit our ability to elucidate the role of SES as a key element of social determinants of health in kidney transplantation. This study's objective was to use an innovative SES measure, the HOUsing-based SES measure (HOUSES) index, to examine the effects of social determinants of health on access to and outcomes of kidney transplantation.
Methods: Our study included residents of Minnesota (age older than 18 y) who underwent kidney transplantation at a single center between 2010 and 2020. SES was determined using the HOUSES index, categorized into quartiles (Q1 for lower, Q2-Q4 for higher SES). We used mixed-effects multivariable logistic and Cox models to examine the effects of HOUSES on preemptive transplants, pretransplant dialysis duration, and death-censored graft loss, adjusting for covariates.
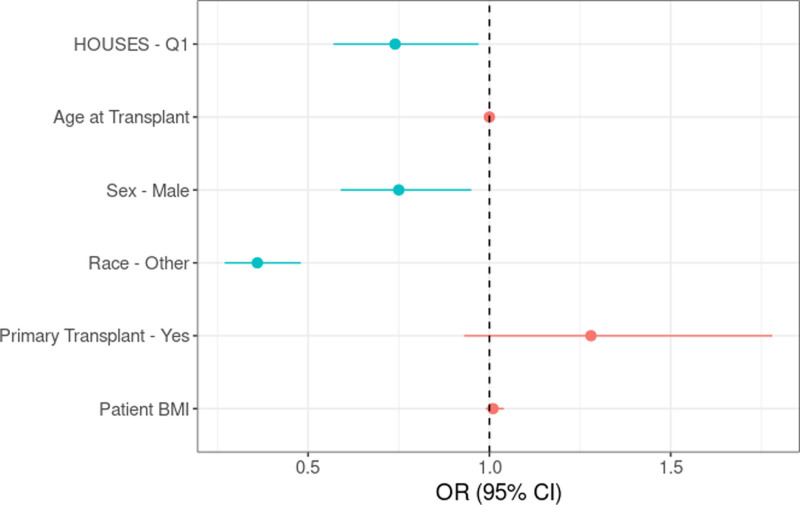
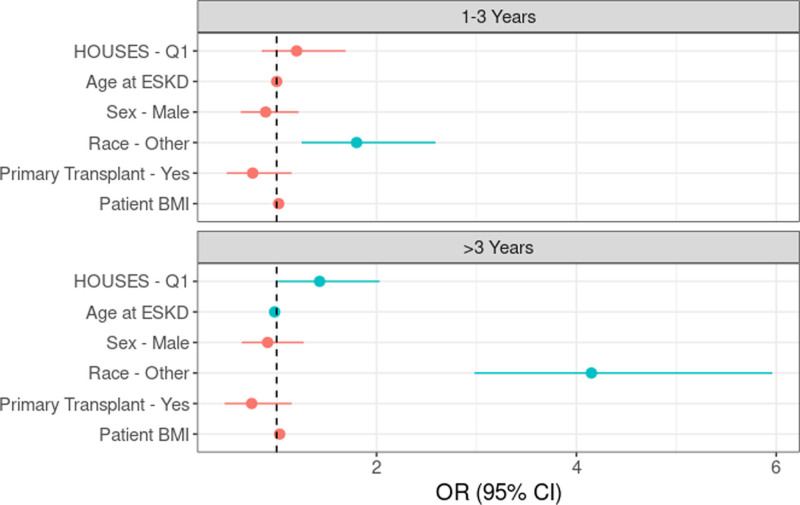
Results: Among 1975 eligible patients, 29.4% received preemptive transplants, 34.9% underwent pretransplant dialysis for >3 y, and 15.1% experienced death-censored graft loss for a median follow-up of 7.15 (interquartile range, 4.25-11.38) y. Lower SES recipients (Q1) demonstrated decreased preemptive transplant likelihood (adjusted odds ratio [aOR]: 0.74; 95% confidence interval [CI], 0.57-0.97; P = 0.03), longer dialysis duration (>3 y; aOR: 1.43; 95% CI, 1.01-2.03; P = 0.046), and higher death-censored graft loss (adjusted hazard ratio 1.36; 95% CI, 1.02-1.12; P = 0.036) versus higher SES recipients (Q2-Q4).
Conclusions: We observed significant socioeconomic disparities in kidney transplant access, dialysis duration, and graft survival. The HOUSES index may be a promising tool for individual-based targeted interventions as it identifies SES on an individual rather than an area-level basis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


