Yangyi Fang, Zhe Zhang, Yinchu Cheng, Zhigao Huang, Jiayuan Pan, Zixuan Xue, Yidong Chen, Vera Y Chung, Li Zhang, Kai Hong
{"title":"Independent factors associated with intracytoplasmic sperm injection outcomes in patients with complete azoospermia factor c microdeletions.","authors":"Yangyi Fang, Zhe Zhang, Yinchu Cheng, Zhigao Huang, Jiayuan Pan, Zixuan Xue, Yidong Chen, Vera Y Chung, Li Zhang, Kai Hong","doi":"10.1093/hropen/hoae071","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>Which independent factors influence ICSI outcomes in patients with complete azoospermia factor c (AZFc) microdeletions?</p><p><strong>Summary answer: </strong>In patients with complete AZFc microdeletions, the sperm source, male LH, the type of infertility in women, and maternal age are the independent factors associated with ICSI outcomes.</p><p><strong>What is known already: </strong>AZF microdeletions are the second most prevalent factor contributing to infertility in men, with AZFc microdeletions being the most frequently affected locus, accounting for 60-70% of all cases. The primary clinical phenotypes are oligoasthenozoospermia and azoospermia in patients with complete AZFc microdeletions. These patients can achieve paternity through ICSI using either testicular (T-S) or ejaculated (E-S) spermatozoa. With aging in men with AZFc microdeletions, oligoasthenozoospermia or severe oligozoospermia may gradually progress to azoospermia.</p><p><strong>Study design size duration: </strong>In this retrospective cohort study, the independent factors associated with the outcomes of 634 ICSI cycles in 634 couples with the transfer of 1005 embryos between February 2015 and December 2023 were evaluated. The analysis included 398 ICSI cycles in 398 couples using E-S and 236 ICSI cycles in 236 couples using T-S; all men had complete AZFc microdeletions.</p><p><strong>Participants/materials setting methods: </strong>The inclusion criteria were as follows: (i) men had complete AZFc microdeletions and (ii) the couple underwent ICSI treatment using T-S or E-S. The exclusion criteria were as follows: (i) cycles involving frozen-thawed oocytes; (ii) cycles in which all fresh embryos were frozen and not transferred; (iii) cycles lost to follow-up; and (iv) multiple ICSI cycles, apart from the first cycle for each couple. The primary outcome was the cumulative live birth rate per ICSI cycle, whereas the secondary outcomes were the clinical pregnancy rate per ICSI cycle, fertilization rate, and the no-embryo-suitable-for-transfer cycle rate (NESTR). Moreover, the maternal and neonatal outcomes were analyzed. Continuous variables showing non-normal distributions were expressed as median and interquartile range and were analyzed using the Kruskal-Wallis test. Categorical variables were expressed as percentages and were analyzed using the χ<sup>2</sup> or Fisher's exact test. Linear and logistic regression models were constructed to assess the independent factors associated with ICSI outcomes.</p><p><strong>Main results and the role of chance: </strong>The T-S group exhibited inferior ICSI outcomes than the E-S group, marked by significantly reduced rates of cumulative live birth, clinical pregnancy, fertilization, high-quality embryos, blastocyst formation, and implantation, with higher NESTRs. However, the miscarriage rate and neonatal outcomes did not significantly differ between the groups. Multivariate linear regression analysis demonstrated that reduced fertilization rates were significantly associated with T-S use (adjusted β, -0.281; 95% CI, -0.332 to -0.229). Multivariate logistic regression demonstrated that increased NESTRs were significantly associated with T-S use (adjusted odds ratio (OR), 4.204; 95% CI, 2.340-7.691), along with uterine anomaly in women (adjusted OR, 2.853; 95% CI, 1.053-7.718), infertility in women with multiple etiologies (adjusted OR, 11.118; 95% CI, 2.034-66.508), and advanced maternal age (adjusted OR, 1.138; 95% CI, 1.029-1.263). The use of T-S (adjusted OR, 0.318; 95% CI, 0.188-0.528), uterine anomaly in women (adjusted OR, 0.263; 95% CI, 0.058-0.852), and increased maternal age (adjusted OR, 0.877; 95% CI, 0.801-0.958) were also associated with decreased clinical pregnancy rates per ICSI cycle. Likewise, lower cumulative live birth rates were associated with T-S use (adjusted OR, 0.273; 95% CI, 0.156-0.468), male LH levels (adjusted OR, 0.912; 95% CI, 0.837-0.990), uterine anomaly (adjusted OR, 0.101; 95% CI, 0.005-0.529), and increased maternal age (adjusted OR, 0.873; 95% CI, 0.795-0.958). No significant differences were observed in the maternal and neonatal outcomes between both groups.</p><p><strong>Limitations reasons for caution: </strong>The study was based on a single-center, retrospective cohort design. The molecular diagnosis of AZFc microdeletions was reliant on loci sY254 and sY255 according to the European Academy of Andrology and European Molecular Genetics Quality Network guidelines. While our findings were based on the clinical phenotypes and laboratory parameters, the abnormalities in the genetic profiles of spermatogenesis and early embryonic development in patients between the T-S and E-S groups have not yet been elucidated.</p><p><strong>Wider implications of the findings: </strong>Our results offer important insights into the independent factors that influence ICSI outcomes in patients with complete AZFc microdeletions. ICSI using E-S is a more favorable therapeutic option for younger patients with AZFc microdeletions and with sperm present in their ejaculate. This study highlights a new direction to investigate the molecular and phenotypic differences between the T-S and E-S groups, which may contribute to the diagnosis and treatment of complete AZFc microdeletions.</p><p><strong>Study funding/competing interests: </strong>This study was supported by Capital's Funds for Health Improvement and Research (2022-2-4094), Beijing Natural Science Foundation (7232203, 7242164), National Key Research and Development Program (2021YFC2700200, 2023YFC2705600), National Natural Science Foundation of China (82301889), Peking University Third Hospital Innovation Transformation Fund (BYSYZHKC2023103), Peking University Third Hospital Clinical Cohort Construction Project (BYSYDL2023016), and Young Elite Scientists Sponsorship Program by CAST (2023QNRC001). None of the authors have any competing interests to declare.</p><p><strong>Trial registration number: </strong>N/A.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2024 4","pages":"hoae071"},"PeriodicalIF":11.1000,"publicationDate":"2024-11-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11652272/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoae071","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Study question: Which independent factors influence ICSI outcomes in patients with complete azoospermia factor c (AZFc) microdeletions?
Summary answer: In patients with complete AZFc microdeletions, the sperm source, male LH, the type of infertility in women, and maternal age are the independent factors associated with ICSI outcomes.
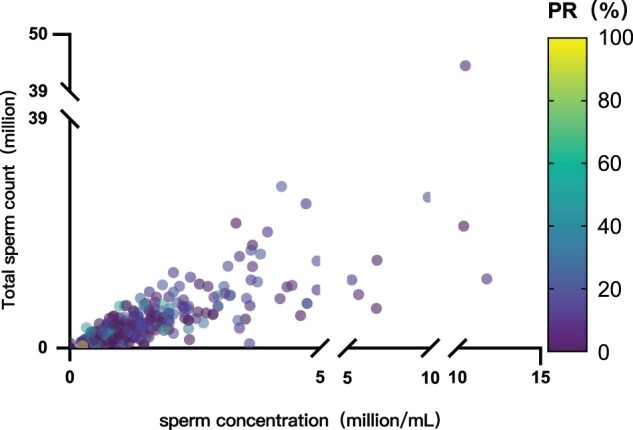
What is known already: AZF microdeletions are the second most prevalent factor contributing to infertility in men, with AZFc microdeletions being the most frequently affected locus, accounting for 60-70% of all cases. The primary clinical phenotypes are oligoasthenozoospermia and azoospermia in patients with complete AZFc microdeletions. These patients can achieve paternity through ICSI using either testicular (T-S) or ejaculated (E-S) spermatozoa. With aging in men with AZFc microdeletions, oligoasthenozoospermia or severe oligozoospermia may gradually progress to azoospermia.
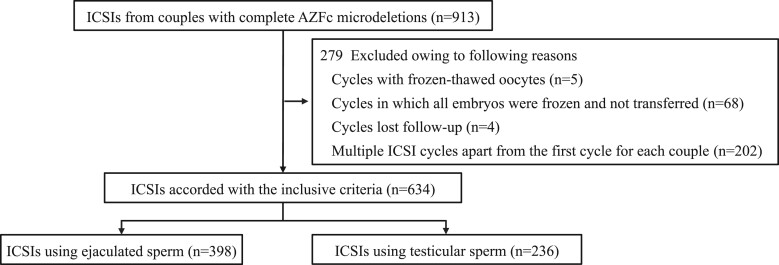
Study design size duration: In this retrospective cohort study, the independent factors associated with the outcomes of 634 ICSI cycles in 634 couples with the transfer of 1005 embryos between February 2015 and December 2023 were evaluated. The analysis included 398 ICSI cycles in 398 couples using E-S and 236 ICSI cycles in 236 couples using T-S; all men had complete AZFc microdeletions.
Participants/materials setting methods: The inclusion criteria were as follows: (i) men had complete AZFc microdeletions and (ii) the couple underwent ICSI treatment using T-S or E-S. The exclusion criteria were as follows: (i) cycles involving frozen-thawed oocytes; (ii) cycles in which all fresh embryos were frozen and not transferred; (iii) cycles lost to follow-up; and (iv) multiple ICSI cycles, apart from the first cycle for each couple. The primary outcome was the cumulative live birth rate per ICSI cycle, whereas the secondary outcomes were the clinical pregnancy rate per ICSI cycle, fertilization rate, and the no-embryo-suitable-for-transfer cycle rate (NESTR). Moreover, the maternal and neonatal outcomes were analyzed. Continuous variables showing non-normal distributions were expressed as median and interquartile range and were analyzed using the Kruskal-Wallis test. Categorical variables were expressed as percentages and were analyzed using the χ2 or Fisher's exact test. Linear and logistic regression models were constructed to assess the independent factors associated with ICSI outcomes.
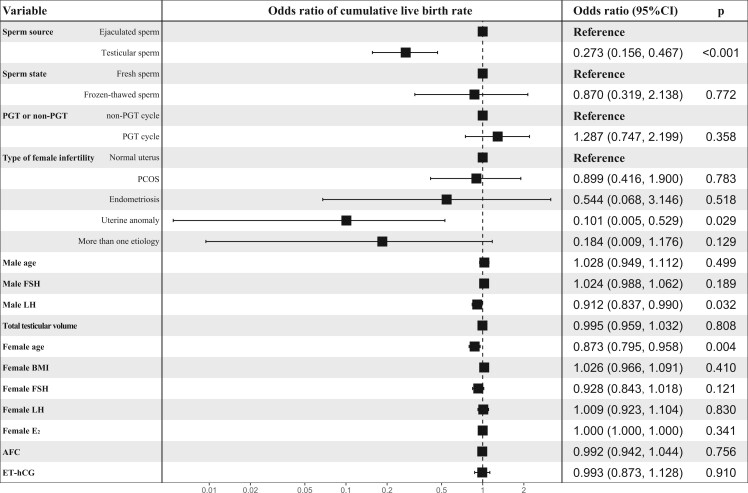
Main results and the role of chance: The T-S group exhibited inferior ICSI outcomes than the E-S group, marked by significantly reduced rates of cumulative live birth, clinical pregnancy, fertilization, high-quality embryos, blastocyst formation, and implantation, with higher NESTRs. However, the miscarriage rate and neonatal outcomes did not significantly differ between the groups. Multivariate linear regression analysis demonstrated that reduced fertilization rates were significantly associated with T-S use (adjusted β, -0.281; 95% CI, -0.332 to -0.229). Multivariate logistic regression demonstrated that increased NESTRs were significantly associated with T-S use (adjusted odds ratio (OR), 4.204; 95% CI, 2.340-7.691), along with uterine anomaly in women (adjusted OR, 2.853; 95% CI, 1.053-7.718), infertility in women with multiple etiologies (adjusted OR, 11.118; 95% CI, 2.034-66.508), and advanced maternal age (adjusted OR, 1.138; 95% CI, 1.029-1.263). The use of T-S (adjusted OR, 0.318; 95% CI, 0.188-0.528), uterine anomaly in women (adjusted OR, 0.263; 95% CI, 0.058-0.852), and increased maternal age (adjusted OR, 0.877; 95% CI, 0.801-0.958) were also associated with decreased clinical pregnancy rates per ICSI cycle. Likewise, lower cumulative live birth rates were associated with T-S use (adjusted OR, 0.273; 95% CI, 0.156-0.468), male LH levels (adjusted OR, 0.912; 95% CI, 0.837-0.990), uterine anomaly (adjusted OR, 0.101; 95% CI, 0.005-0.529), and increased maternal age (adjusted OR, 0.873; 95% CI, 0.795-0.958). No significant differences were observed in the maternal and neonatal outcomes between both groups.
Limitations reasons for caution: The study was based on a single-center, retrospective cohort design. The molecular diagnosis of AZFc microdeletions was reliant on loci sY254 and sY255 according to the European Academy of Andrology and European Molecular Genetics Quality Network guidelines. While our findings were based on the clinical phenotypes and laboratory parameters, the abnormalities in the genetic profiles of spermatogenesis and early embryonic development in patients between the T-S and E-S groups have not yet been elucidated.
Wider implications of the findings: Our results offer important insights into the independent factors that influence ICSI outcomes in patients with complete AZFc microdeletions. ICSI using E-S is a more favorable therapeutic option for younger patients with AZFc microdeletions and with sperm present in their ejaculate. This study highlights a new direction to investigate the molecular and phenotypic differences between the T-S and E-S groups, which may contribute to the diagnosis and treatment of complete AZFc microdeletions.
Study funding/competing interests: This study was supported by Capital's Funds for Health Improvement and Research (2022-2-4094), Beijing Natural Science Foundation (7232203, 7242164), National Key Research and Development Program (2021YFC2700200, 2023YFC2705600), National Natural Science Foundation of China (82301889), Peking University Third Hospital Innovation Transformation Fund (BYSYZHKC2023103), Peking University Third Hospital Clinical Cohort Construction Project (BYSYDL2023016), and Young Elite Scientists Sponsorship Program by CAST (2023QNRC001). None of the authors have any competing interests to declare.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


