Philip J. Koehler III , Paul M. Kitei , David S. Stolzenberg , Elaine H. Hatch
{"title":"Concomitant epidural and longitudinal anterior spinal artery contrast spread in a lumbar transforaminal epidural steroid injection (TFESI)","authors":"Philip J. Koehler III , Paul M. Kitei , David S. Stolzenberg , Elaine H. Hatch","doi":"10.1016/j.inpm.2024.100523","DOIUrl":null,"url":null,"abstract":"<div><div>A 78-year-old female with a remote history of L3-4 decompression and fusion presented with several months of low back and radicular leg pain. MRI revealed moderate L2-L3 spinal canal stenosis, ligamentum flavum infolding, moderate bilateral foraminal stenosis, and a grade I retrolisthesis. A right sided L2-L3 TFESI was performed using multiplanar fluoroscopic imaging with a subpedicular supraneural approach. During live iodinated contrast injection, imaging revealed concomitant epidural and central arterial contrast spread. The needle was retracted and repeat live fluoroscopic imaging demonstrated no vascular uptake. Desired epidural and nerve root contrast spread remained in place with repeat still imaging. Dexamethasone and lidocaine were then injected. The patient suffered no adverse events. This case demonstrates that during a lumbar TFESI, it is possible to have an inadvertent arterial injection with desired epidural contrast spread, despite appropriate needle placement. It emphasizes the importance of necessary precautions, including real-time live fluoroscopy, in order to detect arterial uptake before the delivery of injectate. Without live fluoroscopy, optimal epidural flow at the targeted level can distract interventionalists from the fleeting vascular flow multiple vertebral levels away and risks continuation of the procedure with delivery of injectate.</div></div>","PeriodicalId":100727,"journal":{"name":"Interventional Pain Medicine","volume":"3 4","pages":"Article 100523"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11650285/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interventional Pain Medicine","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2772594424001444","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
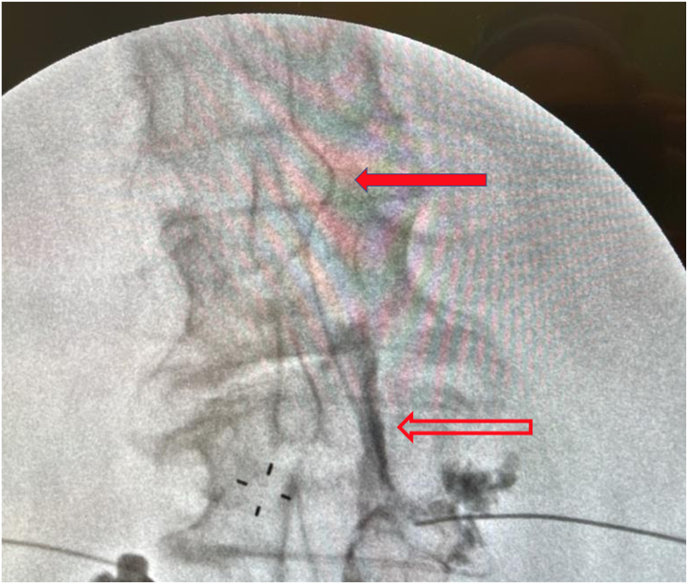
A 78-year-old female with a remote history of L3-4 decompression and fusion presented with several months of low back and radicular leg pain. MRI revealed moderate L2-L3 spinal canal stenosis, ligamentum flavum infolding, moderate bilateral foraminal stenosis, and a grade I retrolisthesis. A right sided L2-L3 TFESI was performed using multiplanar fluoroscopic imaging with a subpedicular supraneural approach. During live iodinated contrast injection, imaging revealed concomitant epidural and central arterial contrast spread. The needle was retracted and repeat live fluoroscopic imaging demonstrated no vascular uptake. Desired epidural and nerve root contrast spread remained in place with repeat still imaging. Dexamethasone and lidocaine were then injected. The patient suffered no adverse events. This case demonstrates that during a lumbar TFESI, it is possible to have an inadvertent arterial injection with desired epidural contrast spread, despite appropriate needle placement. It emphasizes the importance of necessary precautions, including real-time live fluoroscopy, in order to detect arterial uptake before the delivery of injectate. Without live fluoroscopy, optimal epidural flow at the targeted level can distract interventionalists from the fleeting vascular flow multiple vertebral levels away and risks continuation of the procedure with delivery of injectate.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


