Impact of renal-adjusted ceftazidime/avibactam in patients with KPC-producing Klebsiella pneumoniae bloodstream infection: a retrospective cohort study.
A Oliva, L Volpicelli, A Gigante, M Di Nillo, S Trapani, A Viscido, F Sacco, C M Mastroianni
{"title":"Impact of renal-adjusted ceftazidime/avibactam in patients with KPC-producing <i>Klebsiella pneumoniae</i> bloodstream infection: a retrospective cohort study.","authors":"A Oliva, L Volpicelli, A Gigante, M Di Nillo, S Trapani, A Viscido, F Sacco, C M Mastroianni","doi":"10.1093/jacamr/dlae201","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Bloodstream infections (BSIs) caused by KPC-producing <i>Klebsiella pneumoniae</i> (KPC-Kp) are still associated with high mortality, and the game-changing drug ceftazidime/avibactam has shown suboptimal pharmacokinetics in some clinical settings. Ceftazidime/avibactam renal dose adjustment has recently been identified as an independent risk factor for mortality.</p><p><strong>Objectives: </strong>To investigate the effect of ceftazidime/avibactam renal dose adjustment on mortality.</p><p><strong>Methods: </strong>Patients with KPC-Kp BSI treated with a ceftazidime/avibactam-based regimen were retrospectively collected and analysed. The primary outcome was mortality at 7, 14 and 30 days after the start of definitive ceftazidime/avibactam antibiotic therapy. Renal function was estimated using the CKD-EPI equation.</p><p><strong>Results: </strong>One hundred and ten patients with KPC-Kp BSI treated with a ceftazidime/avibactam-based regimen were included. Full-dose ceftazidime/avibactam (7.5 g daily) was prescribed to 82 patients (74.5%), while 28 patients (25.5%) received a renal-adjusted dose (17 patients due to chronic renal disease or haemodialysis, 11 patients due to infection-related acute kidney injury), with a median of 1.9 g daily. At multivariable analysis, receiving a reduced dose of ceftazidime/avibactam was independently associated with mortality (HR 4.47, 95% CI 1.09-18.03, <i>P</i> = 0.037), along with intra-abdominal or lower respiratory tract infections as source of BSI (HR 5.42, 95% CI 1.77-16.55, <i>P</i> = 0.003), septic shock (HR 6.99, 95% CI 1.36-35.87, <i>P</i> = 0.020) and SARS-CoV-2 coinfection (HR 10.23, 95% CI 2.69-38.85, <i>P</i> = 0.001).</p><p><strong>Conclusions: </strong>Dose reduction of ceftazidime/avibactam according to renal function in patients with KPC-Kp BSI seems to be independently associated with higher mortality. This may be possibly due to inadequate exposure provided by the recommended doses for renal impairment.</p>","PeriodicalId":14594,"journal":{"name":"JAC-Antimicrobial Resistance","volume":"6 6","pages":"dlae201"},"PeriodicalIF":3.3000,"publicationDate":"2024-12-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11649808/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAC-Antimicrobial Resistance","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jacamr/dlae201","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Bloodstream infections (BSIs) caused by KPC-producing Klebsiella pneumoniae (KPC-Kp) are still associated with high mortality, and the game-changing drug ceftazidime/avibactam has shown suboptimal pharmacokinetics in some clinical settings. Ceftazidime/avibactam renal dose adjustment has recently been identified as an independent risk factor for mortality.
Objectives: To investigate the effect of ceftazidime/avibactam renal dose adjustment on mortality.
Methods: Patients with KPC-Kp BSI treated with a ceftazidime/avibactam-based regimen were retrospectively collected and analysed. The primary outcome was mortality at 7, 14 and 30 days after the start of definitive ceftazidime/avibactam antibiotic therapy. Renal function was estimated using the CKD-EPI equation.
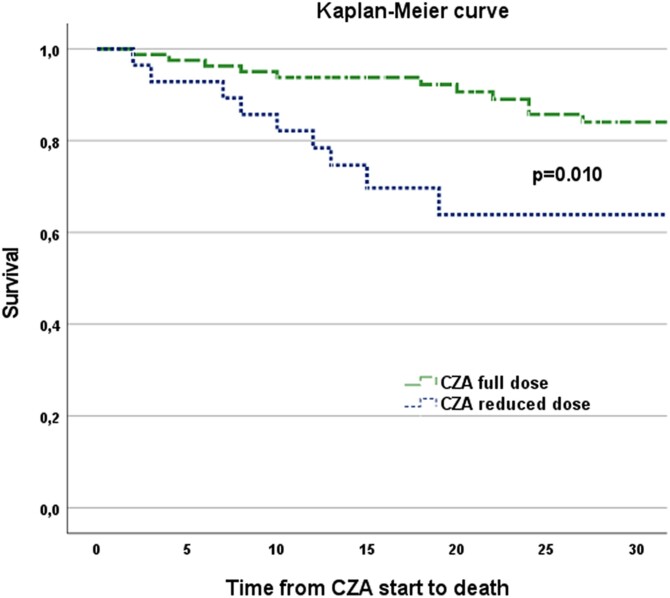
Results: One hundred and ten patients with KPC-Kp BSI treated with a ceftazidime/avibactam-based regimen were included. Full-dose ceftazidime/avibactam (7.5 g daily) was prescribed to 82 patients (74.5%), while 28 patients (25.5%) received a renal-adjusted dose (17 patients due to chronic renal disease or haemodialysis, 11 patients due to infection-related acute kidney injury), with a median of 1.9 g daily. At multivariable analysis, receiving a reduced dose of ceftazidime/avibactam was independently associated with mortality (HR 4.47, 95% CI 1.09-18.03, P = 0.037), along with intra-abdominal or lower respiratory tract infections as source of BSI (HR 5.42, 95% CI 1.77-16.55, P = 0.003), septic shock (HR 6.99, 95% CI 1.36-35.87, P = 0.020) and SARS-CoV-2 coinfection (HR 10.23, 95% CI 2.69-38.85, P = 0.001).
Conclusions: Dose reduction of ceftazidime/avibactam according to renal function in patients with KPC-Kp BSI seems to be independently associated with higher mortality. This may be possibly due to inadequate exposure provided by the recommended doses for renal impairment.
背景:由产生kpc的肺炎克雷伯菌(KPC-Kp)引起的血流感染(bsi)仍然与高死亡率相关,并且改变游戏规则的药物头孢他啶/阿维巴坦在一些临床环境中显示出次优的药代动力学。头孢他啶/阿维巴坦肾剂量调整最近被确定为死亡的独立危险因素。目的:探讨头孢他啶/阿维巴坦肾剂量调整对死亡率的影响。方法:回顾性收集并分析以头孢他啶/阿维巴坦为基础的方案治疗的KPC-Kp BSI患者。主要终点是开始确定头孢他啶/阿维巴坦抗生素治疗后7、14和30天的死亡率。使用CKD-EPI方程估计肾功能。结果:110例KPC-Kp BSI患者接受头孢他啶/阿维巴坦为基础的方案治疗。82例患者(74.5%)使用全剂量头孢他啶/阿维巴坦(7.5 g /天),28例患者(25.5%)接受肾脏调整剂量(17例患者因慢性肾脏疾病或血液透析,11例患者因感染相关急性肾损伤),中位剂量为1.9 g /天。在多变量分析中,接受减少剂量的头孢他啶/阿维巴坦与死亡率(相对危险度4.47,95% CI 1.09-18.03, P = 0.037)、腹腔或下呼吸道感染作为BSI的来源(相对危险度5.42,95% CI 1.77-16.55, P = 0.003)、感染性休克(相对危险度6.99,95% CI 1.36-35.87, P = 0.020)和SARS-CoV-2合并感染(相对危险度10.23,95% CI 2.69-38.85, P = 0.001)独立相关。结论:KPC-Kp BSI患者根据肾功能减少头孢他啶/阿维巴坦的剂量似乎与较高的死亡率独立相关。这可能是由于肾损害的推荐剂量所提供的暴露不足。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


