Eirik Unneland, Anders Norvik, Daniel Bergum, David G Buckler, Abhishek Bhardwaj, Trygve Christian Eftestøl, Elisabete Aramendi, Trond Nordseth, Benjamin S Abella, Jan Terje Kvaløy, Eirik Skogvoll
{"title":"Re-arrest immediately after return of spontaneous circulation: A retrospective observational study of in-hospital cardiac arrest.","authors":"Eirik Unneland, Anders Norvik, Daniel Bergum, David G Buckler, Abhishek Bhardwaj, Trygve Christian Eftestøl, Elisabete Aramendi, Trond Nordseth, Benjamin S Abella, Jan Terje Kvaløy, Eirik Skogvoll","doi":"10.1111/aas.14567","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients who achieve return of spontaneous circulation (ROSC) after in-hospital cardiac arrest (IHCA) may re-arrest. This phenomenon has not been sufficiently investigated. The aim of this study was to examine the immediate (1-min) and short-term (20-min) risks of re-arrest in IHCA.</p><p><strong>Methods: </strong>We retrospectively analyzed four datasets of IHCA episodes, comprising defibrillator recordings collected between 2002 and 2022. Re-arrest was defined as the resumption of chest compressions following a period of ROSC after cardiac arrest of any duration. Parametric models were applied to calculate the immediate risk of re-arrest. In addition, we estimated the short-term risk of re-arrest within 20 min.</p><p><strong>Results: </strong>In 763 episodes of IHCA, we observed 316 re-arrests: 68% to pulseless electrical activity (PEA), 25% to ventricular fibrillation/ventricular tachycardia (VF/VT), and 7% to asystole. Most re-arrests occurred with the same rhythm as in the initial arrest. When ROSC was achieved from a non-shockable rhythm, the risk of re-arrest to a non-shockable rhythm was initially 2% per minute and decreased to 1% per minute after 9 min. The corresponding risk of re-arrest to VF/VT was constant at 2% per minute. If ROSC was obtained from a shockable rhythm, the risk of re-arrest to a shockable rhythm was initially 5% per minute, decreasing to 4% per minute after 9 min. The corresponding risk to a non-shockable rhythm was constant at 1% per minute. The risk of re-arrest within 20 min was 27%, and the overall risk of at least one re-arrest per episode was 33%.</p><p><strong>Conclusions: </strong>The immediate risk of re-arrest was approximately 2% per minute, with the highest risk occurring as a reversion to VF/VT if ROSC was obtained from VF/VT. The risk of re-arrest within 20 min of the initial arrest was 27%, and the overall risk of at least one re-arrest per episode was 33%.</p>","PeriodicalId":6909,"journal":{"name":"Acta Anaesthesiologica Scandinavica","volume":"69 1","pages":"e14567"},"PeriodicalIF":2.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11653231/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta Anaesthesiologica Scandinavica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/aas.14567","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Patients who achieve return of spontaneous circulation (ROSC) after in-hospital cardiac arrest (IHCA) may re-arrest. This phenomenon has not been sufficiently investigated. The aim of this study was to examine the immediate (1-min) and short-term (20-min) risks of re-arrest in IHCA.
Methods: We retrospectively analyzed four datasets of IHCA episodes, comprising defibrillator recordings collected between 2002 and 2022. Re-arrest was defined as the resumption of chest compressions following a period of ROSC after cardiac arrest of any duration. Parametric models were applied to calculate the immediate risk of re-arrest. In addition, we estimated the short-term risk of re-arrest within 20 min.
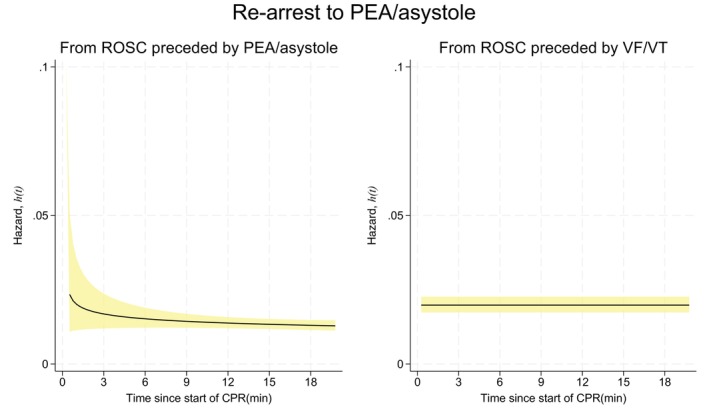
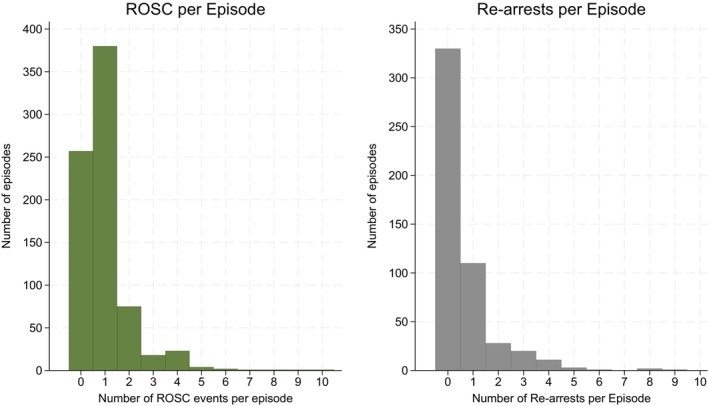
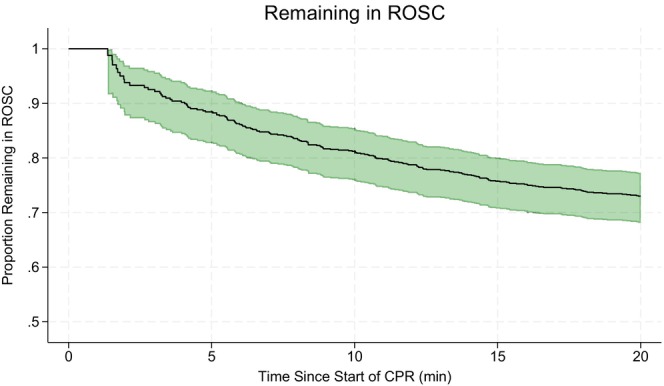
Results: In 763 episodes of IHCA, we observed 316 re-arrests: 68% to pulseless electrical activity (PEA), 25% to ventricular fibrillation/ventricular tachycardia (VF/VT), and 7% to asystole. Most re-arrests occurred with the same rhythm as in the initial arrest. When ROSC was achieved from a non-shockable rhythm, the risk of re-arrest to a non-shockable rhythm was initially 2% per minute and decreased to 1% per minute after 9 min. The corresponding risk of re-arrest to VF/VT was constant at 2% per minute. If ROSC was obtained from a shockable rhythm, the risk of re-arrest to a shockable rhythm was initially 5% per minute, decreasing to 4% per minute after 9 min. The corresponding risk to a non-shockable rhythm was constant at 1% per minute. The risk of re-arrest within 20 min was 27%, and the overall risk of at least one re-arrest per episode was 33%.
Conclusions: The immediate risk of re-arrest was approximately 2% per minute, with the highest risk occurring as a reversion to VF/VT if ROSC was obtained from VF/VT. The risk of re-arrest within 20 min of the initial arrest was 27%, and the overall risk of at least one re-arrest per episode was 33%.
期刊介绍:
Acta Anaesthesiologica Scandinavica publishes papers on original work in the fields of anaesthesiology, intensive care, pain, emergency medicine, and subjects related to their basic sciences, on condition that they are contributed exclusively to this Journal. Case reports and short communications may be considered for publication if of particular interest; also letters to the Editor, especially if related to already published material. The editorial board is free to discuss the publication of reviews on current topics, the choice of which, however, is the prerogative of the board. Every effort will be made by the Editors and selected experts to expedite a critical review of manuscripts in order to ensure rapid publication of papers of a high scientific standard.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


