Vasileios Panagiotopoulos, Ioannis Panagiotis Athinodorou, Kyprianos Kolios, Constantinos Kattou, Andreas Grzeczinski, Andreas Theofanopoulos, Lambros Messinis, Constantine Constantoyannis, Petros Zampakis
{"title":"Microsurgical management of previously embolized intracranial aneurysms: A single center experience and literature review.","authors":"Vasileios Panagiotopoulos, Ioannis Panagiotis Athinodorou, Kyprianos Kolios, Constantinos Kattou, Andreas Grzeczinski, Andreas Theofanopoulos, Lambros Messinis, Constantine Constantoyannis, Petros Zampakis","doi":"10.7461/jcen.2024.E2024.05.004","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Endovascular treatment of intracranial aneurysms (IAs) provides less invasiveness and lower morbidity than microsurgical clipping, albeit with a long-term recurrence rate estimated at 20%. We present our single-center experience and a literature review concerning surgical clipping of recurrent previously coiled aneurysms.</p><p><strong>Methods: </strong>Retrospective analysis of nine (9) patients' data and final clinical/angiographic outcomes, who underwent surgical clipping of IAs in our center following initial endovascular treatment, over a 12-year period (2010-2022). Regarding the literature review, data were extracted from 48 studies including 969 patients with 976 aneurysms.</p><p><strong>Results: </strong>9 patients (5 males - 4 females) were included in the study with a mean age of 49 years. Subarachnoid hemorrhage was the initial presentation in 78% of patients. Aneurysms' most common location was the middle cerebral artery bifurcation (5/9) followed by the anterior communicating artery (3/9) and the internal carotid artery bifurcation (1/9). Indications for surgery were coil loosening, coil compaction, sac regrowth, and residual neck. Procedure-related morbidity and mortality were zero whereas complete aneurysm occlusion was achieved after surgical clipping in all cases (100%). All patients had minimal symptoms or were asymptomatic (mRS 0-1) at the final follow-up.</p><p><strong>Conclusions: </strong>Surgical clipping seems a feasible and safe technique for selected cases of recurrent previously coiled intracranial aneurysms. A universally accepted recurrence classification system and a guideline template for the management of such cases are needed.</p>","PeriodicalId":94072,"journal":{"name":"Journal of cerebrovascular and endovascular neurosurgery","volume":" ","pages":"1-18"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11984270/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cerebrovascular and endovascular neurosurgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7461/jcen.2024.E2024.05.004","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/17 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Endovascular treatment of intracranial aneurysms (IAs) provides less invasiveness and lower morbidity than microsurgical clipping, albeit with a long-term recurrence rate estimated at 20%. We present our single-center experience and a literature review concerning surgical clipping of recurrent previously coiled aneurysms.
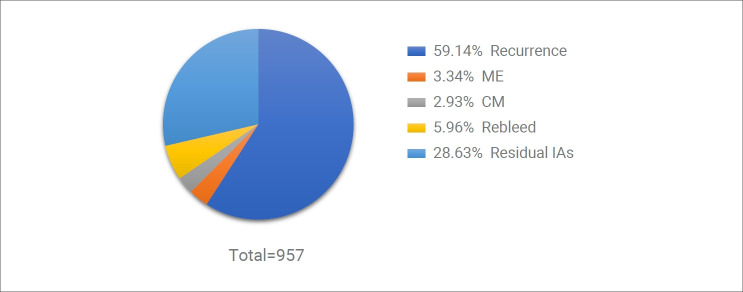
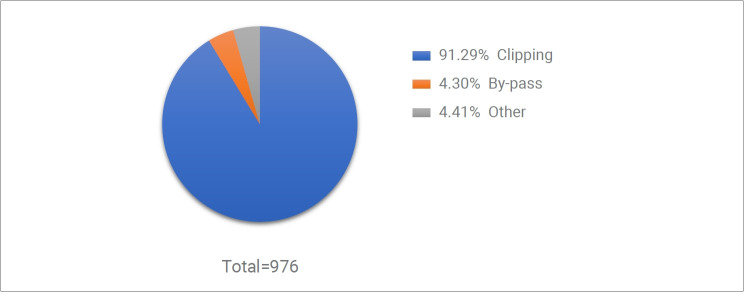
Methods: Retrospective analysis of nine (9) patients' data and final clinical/angiographic outcomes, who underwent surgical clipping of IAs in our center following initial endovascular treatment, over a 12-year period (2010-2022). Regarding the literature review, data were extracted from 48 studies including 969 patients with 976 aneurysms.
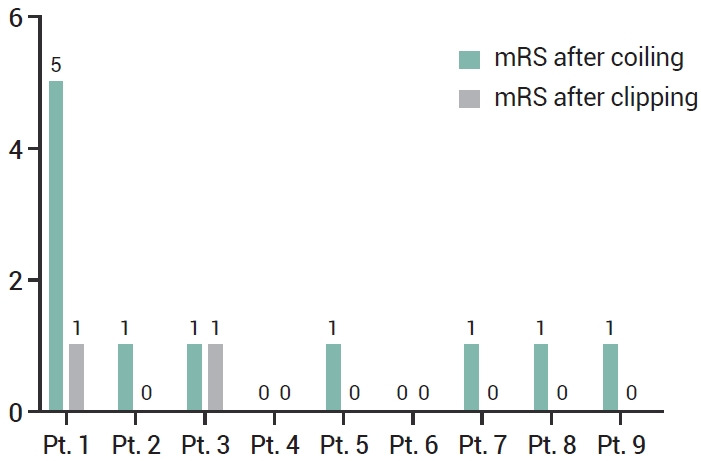
Results: 9 patients (5 males - 4 females) were included in the study with a mean age of 49 years. Subarachnoid hemorrhage was the initial presentation in 78% of patients. Aneurysms' most common location was the middle cerebral artery bifurcation (5/9) followed by the anterior communicating artery (3/9) and the internal carotid artery bifurcation (1/9). Indications for surgery were coil loosening, coil compaction, sac regrowth, and residual neck. Procedure-related morbidity and mortality were zero whereas complete aneurysm occlusion was achieved after surgical clipping in all cases (100%). All patients had minimal symptoms or were asymptomatic (mRS 0-1) at the final follow-up.
Conclusions: Surgical clipping seems a feasible and safe technique for selected cases of recurrent previously coiled intracranial aneurysms. A universally accepted recurrence classification system and a guideline template for the management of such cases are needed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


