Patrick O'Driscoll, David Gent, Liam Corbett, Rod Stables, Rebecca Dobson
{"title":"Feasibility of three dimensional and strain transthoracic echocardiography in a single-centre dedicated NHS cardio-oncology clinic.","authors":"Patrick O'Driscoll, David Gent, Liam Corbett, Rod Stables, Rebecca Dobson","doi":"10.1186/s44156-024-00063-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Following the publication of international cardio-oncology (CO) imaging guidelines, standard echocardiographic monitoring parameters of left ventricular systolic function have been endorsed. Recommendations highlight that either two-dimensional (2D) or three-dimensional (3D) left ventricular ejection fraction (LVEF), alongside global longitudinal strain (GLS) should be routinely performed for surveillance of patients at risk of cancer therapy-related cardiac dysfunction (CTRCD). We studied the feasibility of 3D-LVEF, 2D-GLS and 2D-LVEF in a dedicated CO service.</p><p><strong>Methods: </strong>This was a single-centre prospective analysis of consecutive all-comer patients (n = 105) referred to an NHS CO clinic. Using a dedicated Philips EPIQ CVx v7.0, with X5-1 3D-transducer and 3DQA software, we sought to acquire and analyse 2D- and 3D-LVEF and 2D-GLS, adhering to the British Society of Echocardiography (BSE) and British Cardio-Oncology Society (BCOS) transthoracic echocardiography protocol.</p><p><strong>Results: </strong>A total of 105 patients were enrolled in the study; 5 were excluded due to carcinoid heart disease (n = 5). Calculation of 3D-LVEF was achieved in 40% (n = 40), 2D-GLS in 73% (n = 73), and 2D-LVEF in 81% (n = 81). LV quantification was not possible in 19% (n = 19) due to poor myocardial border definition. Strong correlation existed between 2D-LVEF and 3D-LVEF (r = 0.94, p < 0.0001). Bland-Altman plot demonstrated no statistical differences in that the mean deviation between 2D-LVEF and 3D-LVEF were consistent throughout a range of LVEF values. The most persistent obstacle to 3D-LVEF acquisition was insufficient myocardial border tracking (n = 30, 50%).</p><p><strong>Conclusion: </strong>This study demonstrates the high feasibility of 2D-GLS and 2D-LVEF, even in those with challenging echocardiographic windows. The lower feasibility of 3D-LVEF limits its real-world clinical application, even though only a small difference in agreement with 2D-LVEF calculation was found when successfully performed.</p>","PeriodicalId":45749,"journal":{"name":"Echo Research and Practice","volume":"11 1","pages":"27"},"PeriodicalIF":2.4000,"publicationDate":"2024-12-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11648287/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Echo Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44156-024-00063-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Following the publication of international cardio-oncology (CO) imaging guidelines, standard echocardiographic monitoring parameters of left ventricular systolic function have been endorsed. Recommendations highlight that either two-dimensional (2D) or three-dimensional (3D) left ventricular ejection fraction (LVEF), alongside global longitudinal strain (GLS) should be routinely performed for surveillance of patients at risk of cancer therapy-related cardiac dysfunction (CTRCD). We studied the feasibility of 3D-LVEF, 2D-GLS and 2D-LVEF in a dedicated CO service.
Methods: This was a single-centre prospective analysis of consecutive all-comer patients (n = 105) referred to an NHS CO clinic. Using a dedicated Philips EPIQ CVx v7.0, with X5-1 3D-transducer and 3DQA software, we sought to acquire and analyse 2D- and 3D-LVEF and 2D-GLS, adhering to the British Society of Echocardiography (BSE) and British Cardio-Oncology Society (BCOS) transthoracic echocardiography protocol.
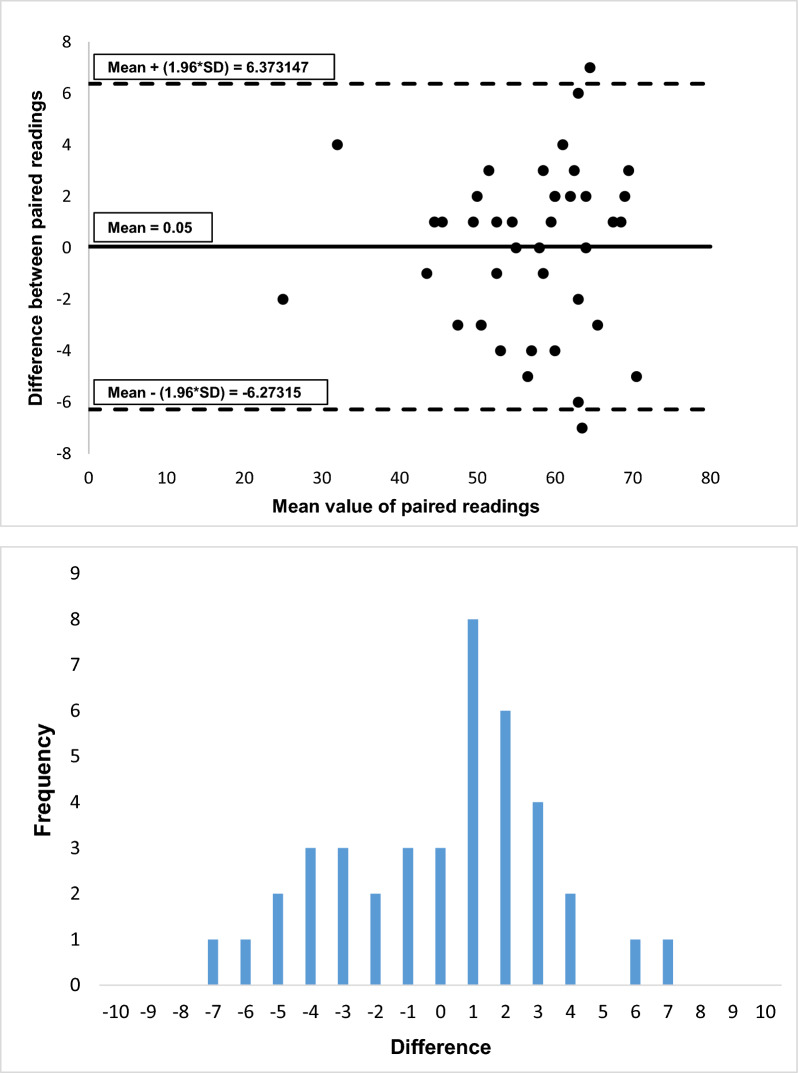
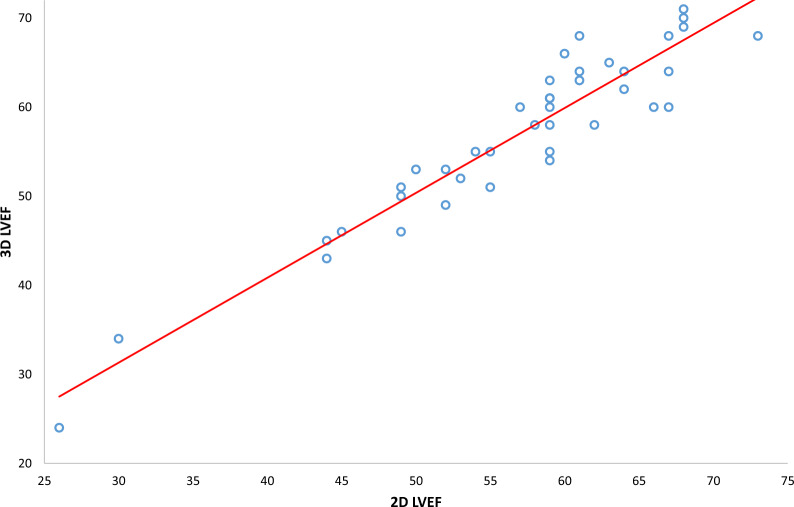
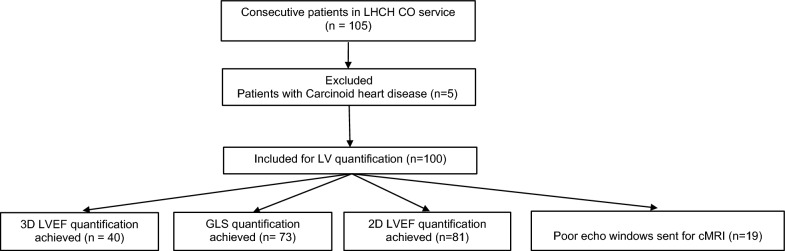
Results: A total of 105 patients were enrolled in the study; 5 were excluded due to carcinoid heart disease (n = 5). Calculation of 3D-LVEF was achieved in 40% (n = 40), 2D-GLS in 73% (n = 73), and 2D-LVEF in 81% (n = 81). LV quantification was not possible in 19% (n = 19) due to poor myocardial border definition. Strong correlation existed between 2D-LVEF and 3D-LVEF (r = 0.94, p < 0.0001). Bland-Altman plot demonstrated no statistical differences in that the mean deviation between 2D-LVEF and 3D-LVEF were consistent throughout a range of LVEF values. The most persistent obstacle to 3D-LVEF acquisition was insufficient myocardial border tracking (n = 30, 50%).
Conclusion: This study demonstrates the high feasibility of 2D-GLS and 2D-LVEF, even in those with challenging echocardiographic windows. The lower feasibility of 3D-LVEF limits its real-world clinical application, even though only a small difference in agreement with 2D-LVEF calculation was found when successfully performed.
期刊介绍:
Echo Research and Practice aims to be the premier international journal for physicians, sonographers, nurses and other allied health professionals practising echocardiography and other cardiac imaging modalities. This open-access journal publishes quality clinical and basic research, reviews, videos, education materials and selected high-interest case reports and videos across all echocardiography modalities and disciplines, including paediatrics, anaesthetics, general practice, acute medicine and intensive care. Multi-modality studies primarily featuring the use of cardiac ultrasound in clinical practice, in association with Cardiac Computed Tomography, Cardiovascular Magnetic Resonance or Nuclear Cardiology are of interest. Topics include, but are not limited to: 2D echocardiography 3D echocardiography Comparative imaging techniques – CCT, CMR and Nuclear Cardiology Congenital heart disease, including foetal echocardiography Contrast echocardiography Critical care echocardiography Deformation imaging Doppler echocardiography Interventional echocardiography Intracardiac echocardiography Intraoperative echocardiography Prosthetic valves Stress echocardiography Technical innovations Transoesophageal echocardiography Valve disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


