{"title":"An Atypical Presentation of Acute Cholecystitis with Left Sided Chest Pain and ST Elevation - A Case Report.","authors":"Helene G Meyer, Kristina Fäh, Michael Christ","doi":"10.2147/OAEM.S478102","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>ST elevation combined with typical chest pain is an indication for acute coronary vascularization and is usually associated with acute myocardial infarction. Herein, we present an unusual case of ST elevation.</p><p><strong>Case presentation: </strong>A 57-year-old male patient presented to the emergency department with chest pain radiating to both arms and the back. Typical clinical presentation and inferolateral ST elevations were suggestive of ST elevation myocardial infarction. Interestingly, coronary occlusion was excluded by coronary angiography. Despite extensive diagnostic workup, no underlying diagnosis was made. Four days later, the patient returned and reported pain in the right upper abdomen. Clinical presentation, laboratory analysis, and imaging features led to a diagnosis of calculous acute cholecystitis. Laparoscopic cholecystectomy was performed, and the diagnosis was confirmed. Electrocardiographic changes and pain resolved completely.</p><p><strong>Conclusion: </strong>Acute calculous cholecystitis is initiated by gallbladder distension due to biliary duct occlusion caused by gallstones. ST elevations in response to gallbladder distension have been demonstrated in animal models. We hypothesize that the ST elevations observed in this patient with chest pain were linked to stone-mediated distension of the gallbladder, leading to reflex coronary vasoconstriction.</p>","PeriodicalId":45096,"journal":{"name":"Open Access Emergency Medicine","volume":"16 ","pages":"323-328"},"PeriodicalIF":1.5000,"publicationDate":"2024-12-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11638474/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S478102","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: ST elevation combined with typical chest pain is an indication for acute coronary vascularization and is usually associated with acute myocardial infarction. Herein, we present an unusual case of ST elevation.
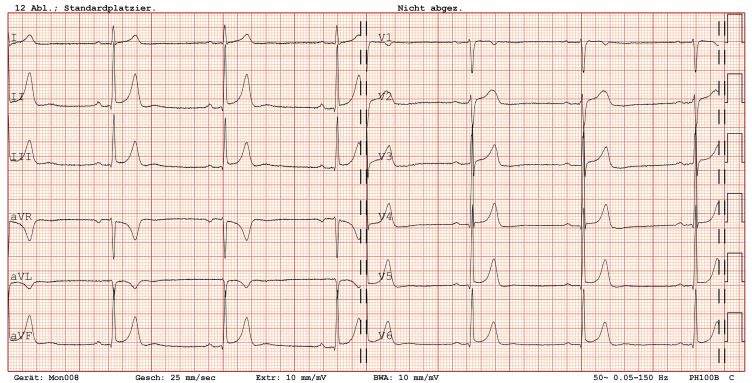
Case presentation: A 57-year-old male patient presented to the emergency department with chest pain radiating to both arms and the back. Typical clinical presentation and inferolateral ST elevations were suggestive of ST elevation myocardial infarction. Interestingly, coronary occlusion was excluded by coronary angiography. Despite extensive diagnostic workup, no underlying diagnosis was made. Four days later, the patient returned and reported pain in the right upper abdomen. Clinical presentation, laboratory analysis, and imaging features led to a diagnosis of calculous acute cholecystitis. Laparoscopic cholecystectomy was performed, and the diagnosis was confirmed. Electrocardiographic changes and pain resolved completely.
Conclusion: Acute calculous cholecystitis is initiated by gallbladder distension due to biliary duct occlusion caused by gallstones. ST elevations in response to gallbladder distension have been demonstrated in animal models. We hypothesize that the ST elevations observed in this patient with chest pain were linked to stone-mediated distension of the gallbladder, leading to reflex coronary vasoconstriction.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


